
Must see update to a previous blog at the end of this blog entry.
Mass vaccination doesn’t work, as a comparison between two contrasting states indicates. Vermont is the most vaccinated state in the country, with more than 70 percent of the population fully vaccinated. Despite this, they are in the midst of a the worst COVID-19 surge in the nation. Indeed, COVID-19 cases are more numerous in Vermont than at any time during the entire pandemic for that state.


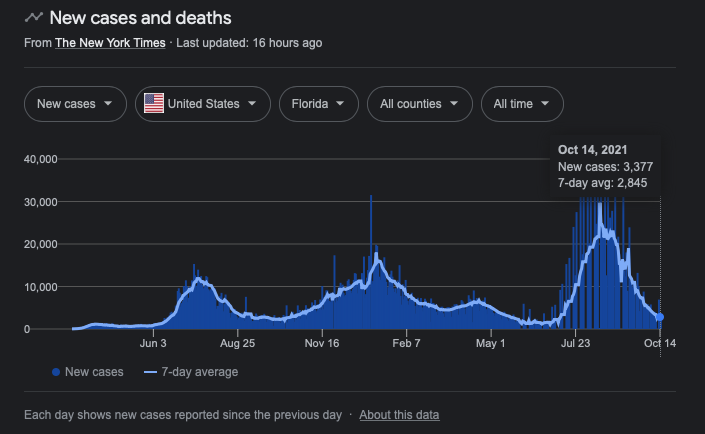
In contrast, Florida’s last COVID-19 surge peaked almost two months ago. Today, the average per capita new coronavirus cases in Florida are the lowest of any state in the nation. Florida has received extraordinary levels of negative media coverage concerning its rate of vaccination (still less than 60 percent, and only 50 percent when the surge peaked), as well as its reluctance to aggressively pursue masking and other draconian pandemic measures seen in other states. One might wish to pull more states into the comparison, but, frankly, on its face, the Vermont case proves that mass vaccination, aggressive masking, etc., don’t work. I will nonetheless provide Florida’s statistics for comparison.

Why don’t the pandemic measures work? I have explained this in several posts on Freedom and Reason. To recap, the mRNA technology is not a vaccine. It is gene therapy and it does not confer immunity. Those injected with the spike protein are able to contract and spread the virus. Because the mRNA injections may reduce the frequency of severe COVID-19, those who have had the shots and are infected may feel well enough to move about the community and spread the virus. This spread also has implications for pathogenesis and evolutionary paths of mutation (or variants). Moreover, despite reducing the risk of severe COVID-19, those who have been injected are still getting severe COVID-19, are hospitalized, and will die of the disease. Indeed, as the proportion of populations who are vaccinated increase, an increasing proportion of severe COVID-19 cases, hospitalizations, and deaths are those who will have received the recommended injections. Don’t fall for the spin about this. There is an attempt to use this fact to rationalize the failure of the vaccines to protect the population from SARS-CoV-2 infection. It is an indictment of mass vaccination.
As evidence makes clear, natural immunity provides more powerful protection in terms of levels of antibodies (as much as 27 times the early protection associated with the injections), and since natural infection exposes the body to the entire pathogen signature, greater diversity of antibodies. Furthermore, research on a number of therapeutics, for example ivermectin, have demonstrated significant efficacy in preventing the development of severe COVID-19 cases in those who are infected and as a prophylaxis in the general population.
Finally, as noted if the vaccines make it less likely for the infected to suffer symptoms that will keep them at home, they are more likely to be about the community spreading the virus. That’s the obvious reason why we are seeing these patterns The less obvious reason is that the vaccine changes the evolutionary trajectory of the pathogen. It allows more pathological variants to last longer in the population, which increases the likelihood of more deleterious mutations. This is why vaccinating in the teeth of a panic is a bad idea. Pathogens leverage population-wide attempts to defeat them by pursuing alternative selection paths. It’s evolutionary biology 101.
* * *
Scott Hurley of Fox News (local Green Bay) authored a story yesterday with this shocking headline: “Unvaccinated 19x as likely to die of COVID compared to vaccinated in Wisconsin.” The headline is nearly identical to headlines rolled out across the country, the frame provided by the CDC (who you will see in the next section are keen on selectively focusing on data and interpretation). They are trying to scare more people into vaccination.
Read beyond the headline and do some math. Of every 100,000 people who were not fully vaccinated, Wisconsin Department of Health Services data shows that 24.5 died from COVID-19. That’s out of 2,351 positive cases, yielding a case fatality rate (CFR) of one percent. Multiply the CFR by five to determine the approximate infection fatality rate (IFR). This yields an IFR of 0.2 percent or two persons for every 1000 SARS-CoV-2 infections. Instead of putting the headline in those risk terms, the reporter ran with 19 times more likely to die than the vaccinated. Given that people drastically overestimate the number of people who die from COVID-19 (as I have shown on this blog), the headline is fear-mongering.
* * *
The prevalence of type-2 diabetes in COVID-19 patients is as high as 36 percent—more than a third of cases. Insulin resistance is not the only consequence of obesity. These patterns are seen worldwide. So why was the pandemic so bad in the United States? Travelling around continental Europe will really bring this home to you. America’s obesity problem has caught up with us. We have to stop denying biological realities. Postmodernist epistemology is wrecking scientific literacy. Type 2 Diabetes Mellitus and COVID-19.
* * *
Update on my blog from a month ago, September 15, 2021, Is the CDC Concealing Deaths from Influenza and Pneumonia? I showed that, according to the CDC’s own data, 47 percent of COVID-19 deaths 2020/2021 to date of data collection for chart production associated with influenza and pneumonia.
In my last blog Faking Genius for Power and Profit, I showed you that coronavirus was known by that name since the early 1960s. There has been no routine testing for coronavirus historically. It’s a cold virus, like adenovirus and rhinovirus. They don’t routinely test for those, either. Why? Because they aren’t a big deal.
The authors are telling us that influenza cases are the lowest in recorded history. If so, then how could influenza and pneumonia have contributed to the deaths of more than 300,000 COVID-19 patients? Is it not possible that we have been through one of the most lethal flu seasons but that, because of a test for coronavirus and the act of prioritizing the coronavirus over influenza to push a novel vaccine, mRNA technology developed on the basis of gain-of-function research in Wuhan, China, research funded by the same crowd (Fauci et al.) who push out the COVID-19 narrative, flu and pneumonia deaths are being portrayed as coronavirus deaths? We can’t say misidentified since the statistic is right there in the table.

We can’t believe masks prevented influenza but not coronavirus. It doesn’t work like that. Influenza didn’t go away. It’s not the lowest level of flu since we starting keeping records. It’s the way the data are represented to the public. The chart I am using is real. You can see it in the blog I cite above. I saved the document in case the CDC purges it. I was shocked to find it, frankly. I was even more shocked to find, when I checked yesterday to see if it was still there, that it is still there—only updated! Here’s the updated chart:
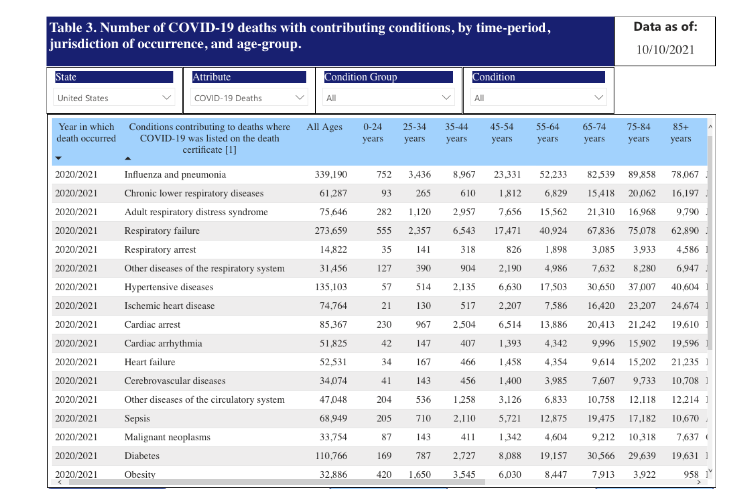
Look at the first line under the blue header bar. Influenza and pneumonia account for 339,190 of COVID-19 deaths as of October 10, 2021. Again, this is the same document as cited in my original blog. Why is the CDC openly publishing these data while simultaneously telling the public that influenza in the United States is at an all-time low?
