In a recent blog (The Establishment Media Running Down the US Pandemic Performance) I noted that four counties—France, Italy, Spain, and the United Kingdom—had death rates comparable to those of the United States. I used the similarities to push back against the establishment media claim that the United States is an outlier in COVID-19 deaths, a claim used to attack the president.
The World Health Organization is expressing concern that COVID-19 cases are rising in Europe (The new Covid-19 case surge in Europe, explained). They have declared it a “very serious situation.” The four countries I used in my comparison are among the affected nations. I present the change over time in four graphs below, obtained by searching “COVID-19 cases [country name].”
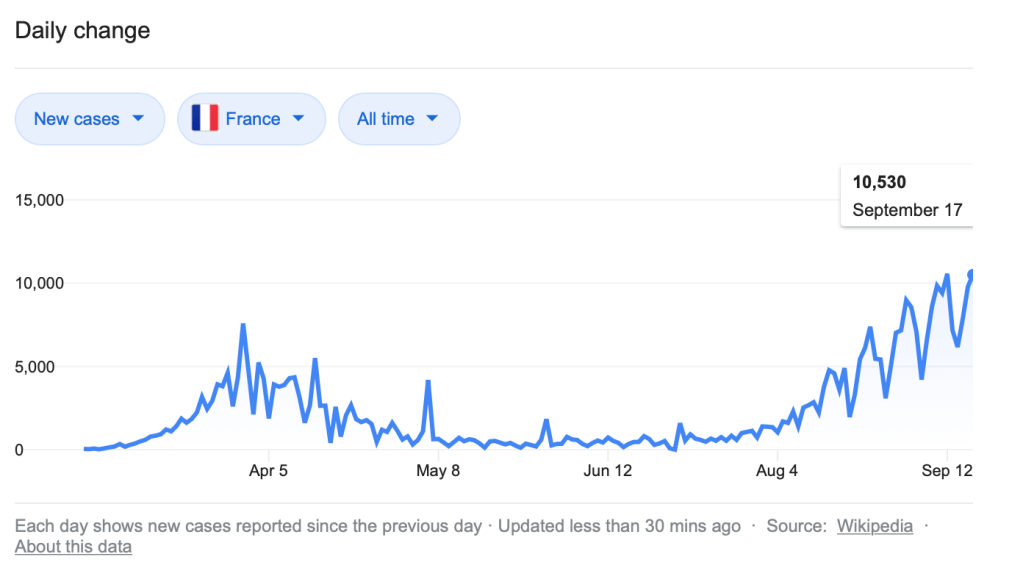
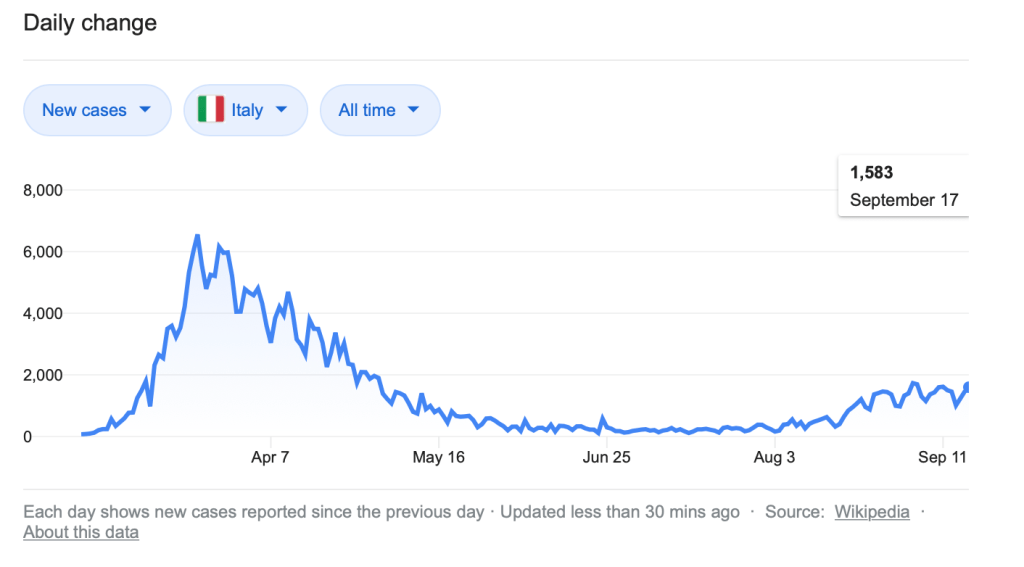
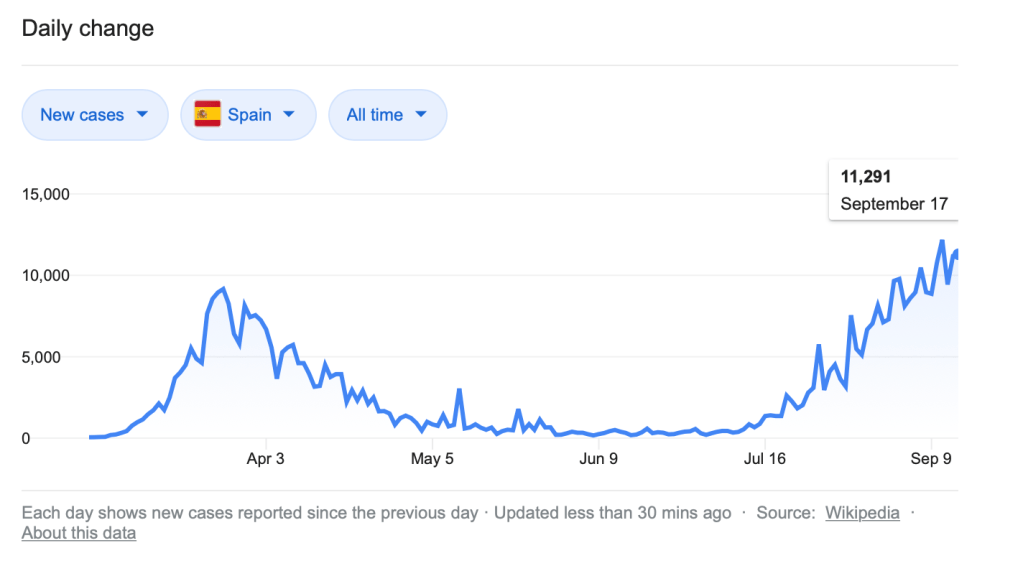
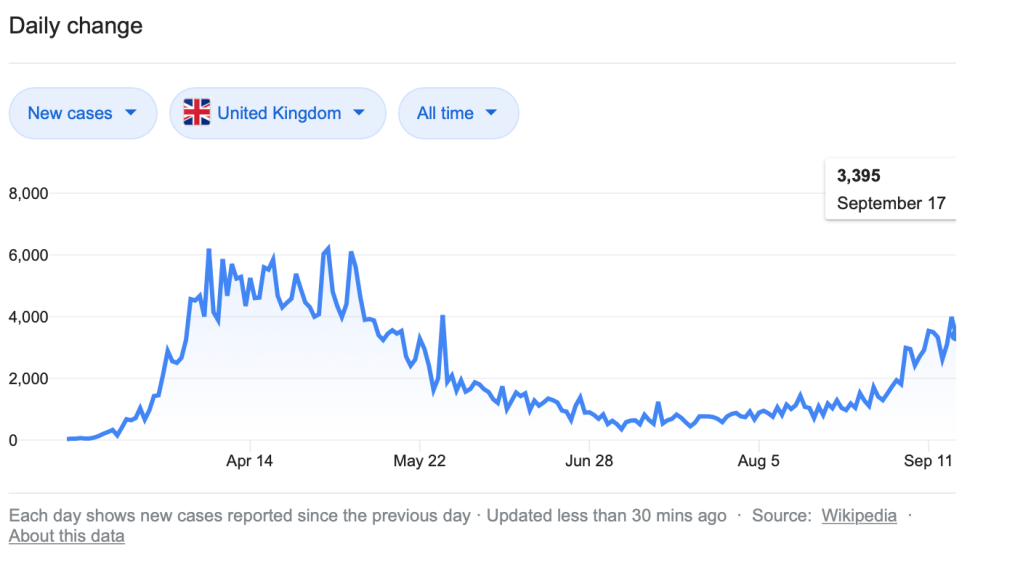
We see that COVID-19 cases are on the rise in all four countries, most drastically in France and Spain, where the current number of cases is higher that the previous peak, which occurred months earlier. For these countries, the rise in cases started back in July. For Italy and the United Kingdom, increasing frequencies becomes clear by early August.
With the warning lights going off, we need to step back and ask the most important question: are the increases in cases associated with increasing deaths? After all, if we tested for any virus and found a growing number of cases we would need to have some reason for this to cause alarm other than the mere presence of a virus. Most viruses are not particularly lethal or even consequential. For example, rhinoviruses are common in human societies yet we don’t test for them nor do we panic when we perceive colds are appearing with greater frequency. The next four charts document the frequency of death in these four European countries.




In only one country (Spain) does it appear that deaths are on the rise in any significant number, and this is the country with the greatest number of new cases. To be sure, if deaths follow, a lag in frequency is expected. Yet, in France, where a dramatic rise in cases began in mid-July, we see only a slight uptick on in the second week of September. Moreover, both Italy and the United Kingdom show very little increase in deaths despite a steady rise in cases. Perhaps this will change over time, but at present it does not appear they rise in cases is associated with increasing death.
Let’s take a look at the United States, where frequency of cases has been much greater since June. As you can see, this is associated with a rise in the frequency of deaths, but the visual comparison is striking in how the number of cases of death was much greater during the period with fewer cases of infection than in the period with more cases of infection.
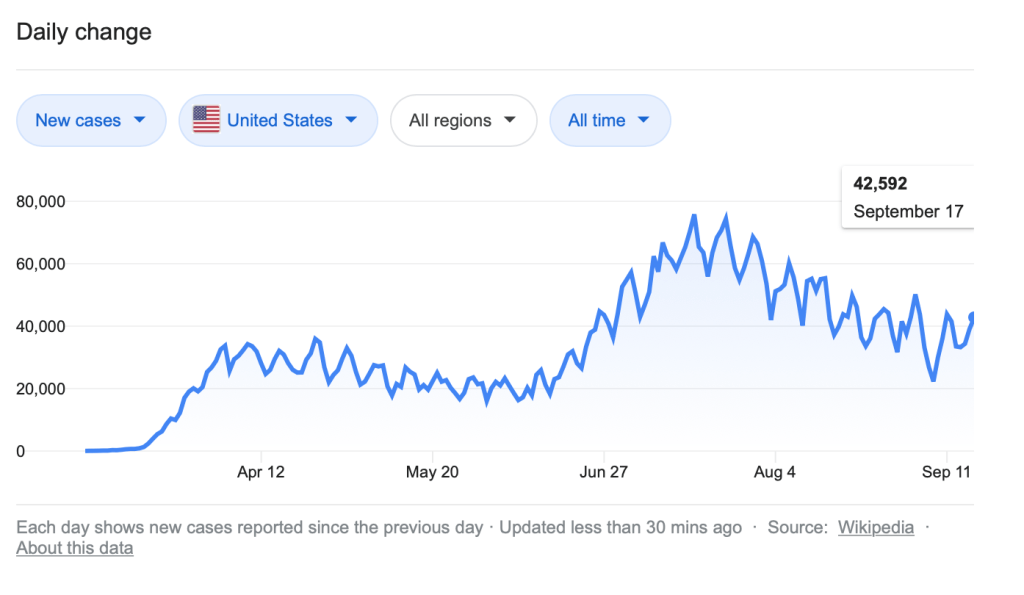
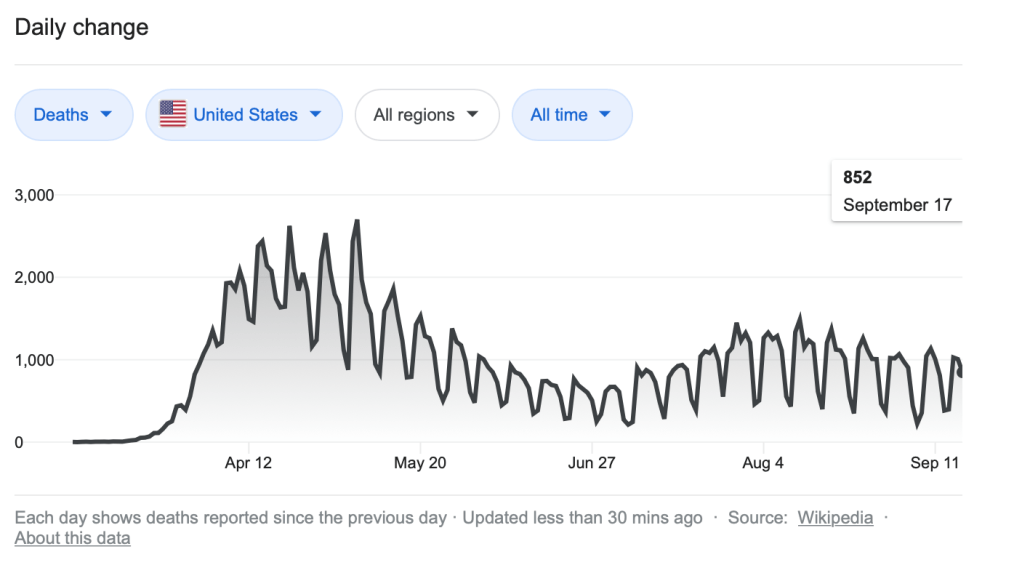
What are we to make of this? Why was there so much greater death in the earlier periods than in the later periods? One reason for this is likely aggressive testing. The more testing authorities do the more cases we uncover, which in turn increases case frequencies. In may be that, in the early months of the pandemic, many more people had the virus that we thought but, with testing constrained, few cases were uncovered, thus producing a much higher case fatality rate, which created the exaggerated perception of the virus’ lethality. As testing ramped up, we began to develop a better understanding of the virus’ true lethality, which was not nearly as great as we initially thought.
This is, of course, assuming the virus has a stable rate of death. Natural history suggests that this is a bad assumption. In nature, the proliferation of virus depends on its successful replication. If, in the replication process, a virus sickens its host to the point where the host cannot effectively spread the virus, then this particular variation cannot spread as effectively as those variations that do less damage to the host. A virus is not trying to sicken or kill its host. It is simply trying to exploit the host’s cellular machinery. With the proliferation of less lethal varieties of SARS-CoV-2, death rates fall while infection rates rise.
It is likely that all of these are simultaneously occurring. There were early on certainly more cases than were detected by testing. The initial case fatality rates were thus based on underreporting of cases. I knew this at the time and reported on it my blog. But the viruses has under evolutionary pressures attenuated over time. It is less lethal than it was before. A rise in cases accompanied by a drastic decline in cate fatality rates should be cause to celebrate, but the establishment media and medical-industrial complex are spinning the statistics in a manner that at least functions to frighten the public. They have switched from death counts to case counts. They are hiding the good news for political purposes.
It may be that the lethality of the virus was magnified by those who were most likely to die from it, namely the old and the infirm. Of the 182,095 deaths recorded by the CDC to date, 104,661, or 57.5 percent, were over age of 74. Including those in the 65-74 age range raises the number to 143,790, increasing the percentage to 79 percent. Including those 55-64 accounts for more than 90 percent of fatalities. Approximately half of all those who died were in long-term care facilities, so it was not just age but health condition. For the other four-fifths of the population, 14,871 died from COVID-related causes. That is two percent of all causes for those age groups. For schools aged children, from daycare through undergraduate, COVID-19 related deaths account for just 1 percent of all deaths for those age groups. (All these stats are from the most recent CDC provisional death reports.)
In late August, data from the Centers for Disease Control and Prevention (CDC) suggested that only 6 percent of people who died of COVID-19 actually have COVID-19 as the sole diagnosis on their death certificate. This isn’t just an issue when COVID-19 is a factor. Underlying diabetes, coronary artery disease, etc., are common diseases that contribute to mortality, They are triggered by influenza, pneumonia, or some other infectious process. When doctors talk about “triggers,” they mean the proximate cause of death. Unfortunately, the media is not educating the public about proximate and ultimate causes.
If you are healthy, a cold virus won’t kill you. Indeed, getting cold viruses as you mature will protect you against cold viruses throughout your life. This improves your quality of life. But if you are very old, with late-stage cancer, have health problems associated with obesity, etc., with an immune system in decline or depleted, then you might not be able to fight off the cold virus. The cold virus is the proximate cause of your death. But the ultimate cause is something on that list I just enumerated. Eventually, sooner than later, all those with underlying conditions will die and their death will likely be the ultimate cause of their death (if they aren’t hit by a bus, struck by lightning, slip in the bathtub, murdered, etc.). The virus—the trigger— could be a rhinovirus, a coronavirus, or some other virus. The point is that the virus is not the ultimate cause of death because it rarely kills anybody by itself. If it does kill somebody by itself, then a deeper investigation is warranted. The doctors missed something. Or foul play is suspected.
Consider a man who has been shot in the chest. He survives, but the injury exposed him to an antibiotic resistant bacteria that invaded his lungs. Should we absolve the man who shot him of murder because the proximate cause of death is a bacterial infection? No, because the ultimate cause of his death is the gunshot wound to his chest. The man who shot him is responsible for this death. His ultimate passing was triggered by the bacterial infection.
The establishment is using a COVID-19 diagnosis in counting deaths to leave the impression that each of us share the same risk of death if we contract SARS-CoV-2. In fact, most of us who are infected won’t even present with symptoms. Half of us probably already have an immunity to the virus because of a lifetime of exposure to coronaviruses (T-cells exhibit cross-immunity). Indeed, the perception conveyed by the media is so false that any expert who does not make sure the public understands this is lying to them. Virtually everybody the media puts in front of you is lying to you. And they’ve been actively censoring those contradicting the official science on this matter. The good news is that you don’t need to be a virologist to understand the logic of science. You just need to be a scientist or think like a scientist.
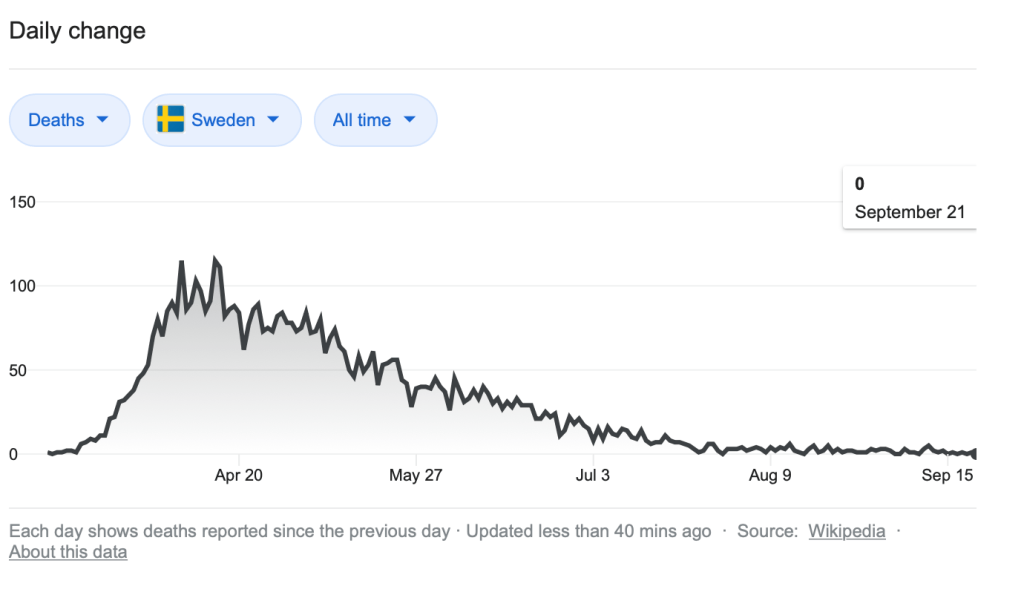
Finally, a comparative point. Sweden pursued a different strategy in handling COVID-19. They sought to build herd immunity while mitigating the worst effects of the disease and thus soften its impact. As you can see by the numbers, this was a sound choice. They are not seeing the rise in cases that the other European countries cited are seeing. There almost no deaths from COVID-19 in Sweden, a diverse country of ten million people.