On the podcast Triggernometry, during a debate with Kellie Jay Keen, Helen Webberley, a former physician and now queer activist, said something quite revealing about gender identity doctrine (a link to the debate follows this essay). She said that gender identity is fixed at birth (or possibly conception, though “we don’t know,” she admitted). Whatever one’s body looks like, it’s the body of one’s gender identity, she explained, which is something one is born with. Bodies don’t matter. It’s the gender identity that determines the person’s gender. If that sounds circular, that’s because it is. But let’s set that problem aside for a moment.
Helen Webberley
Konstanine Kisin, who moderated the debate, brought up a former guest, the transman Buck Angel, who, while appearing as a male, would not have a body identical to Kisin’s since he had a vagina. He brought this up because Webberley had said that a transman is indistinguishable from a cisman. Kisin said they could not be indistinguishable since Angel has a vagina. Webberley insisted that Angel is a man with a vagina. Some men have vaginas, in her worldview. In fact, some men not only have vaginas, but they also have breasts and all the rest of it. That doesn’t make them women. It all goes back to gender identity. Nothing is really fixed except that.
Notice how Webberley assumes gender identity. It is an article of faith that undergirds the doctrine. How would we know Angel has always been a man? Because he tells us he is? People tell others all sorts of things. A child might tell us he is a cat. It would be naive to accept the child’s claim at face value. He may be pretending he is a cat, but he is not. And we have objective ways of testing his claim.
Keen wonders whether there is some test to see whether gender identity is real. Webberley obscures this point by talking about the surgical procedure appendectomy. Doctors aren’t always sure that a person is suffering from appendicitis (and apparently, in roughly 40 percent of the cases, they are not). Webberley would like for us to accept that, since, like appendicitis, we do not always know for sure whether something is real, it is okay to alter bodies with drugs, hormones, and surgeries.
She seems to think the appendectomy case is analogous to gender identity, even while admitting that there are objective metrics that help doctors feel more confident about whether an appendectomy is necessary, such as white blood cell count. She also skirts the fact that appendicitis is an emergency situation in which committing a Type I error, i.e., removing a healthy appendix by mistake, outweighs the risk of a Type II error, i.e., missing a diseased appendix and sending a patient home. Doctors prefer a Type I error because a burst appendix is deadly.
How is that the same as gender identity—especially since Webberley argues that there is nothing to be fixed about the body in the case of gender dysphoria unless the individual wants to change his body? It’s a bad analogy. It is the only analogy she could conjure.
It was disappointing that neither Kisen nor Keen noted the problems with her analogy. However, the question remains: is there an objective metric for diagnosing gender identity? Of course, there isn’t. Gender identity is a subjective thing and therefore unfalsifiable. It exists only in the minds of those who claim it and the industry that invented it.
If we hold Webberley to the claim that gender identity is what determines a person’s sex, not gametes, chromosomes, or reproductive anatomy, then her entire argument for endocrinological and surgical intervention collapses. It’s important to understand Webberley’s argument to see why. Sorry if this sounds repetitive, but this is the crux of the matter so it needs crystal clarity.
From Webberley’s worldview, a boy can be born with what appears to be a girl’s body. But it’s not a girl’s body; it’s a boy’s body because his gender identity is that of a boy. This identity is innate and fixed. For Webberley, that is the truth of the matter. Those who think it’s a girl’s body—like the doctor who wrongly assigned sex at birth—are in error since boys can have bodies that look like those of girls. Put simply, a boy is a boy whatever his body looks like.
If this is true, why transition the boy to make his body look like a boy’s body? Boys’ bodies can naturally look like girls’ bodies, so what needs to be changed? A boy can have small, feminine hands. He already looks like what he is.
“Because the boy feels uncomfortable looking like a girl.” Oh horror. Girls’ bodies are so awful. Misogyny aside, would it not be better to help the boy negotiate his dysphoria by understanding that boys’ bodies can look like girls’ instead of pursuing radical medical measures that will rob him of sexual function and make him a lifelong medical patient?
The boy has internalized a cultural stereotype of how boys should look. Isn’t the queer argument that such expectations are oppressive? Why change his body with puberty blockers, cross-sex hormones, and surgeries if by definition he already has the body of a boy? He won’t ever have a penis, but that’s okay because some boys don’t have penises. Some boys have vaginas instead. They have boy vaginas. It’s just a range of variation.
This is the problem with the prefix “trans.” If gender identity is fixed at birth, then the boy is not changing his identity, only his appearance, and therefore isn’t trans, which literally means “across, beyond, or through.” There is nothing to get across to or beyond. There is nothing to push through. He is already on the correct side. If boys can have vaginas, they aren’t trans anything. They are simply boys with vaginas.
I am sure Webberley did not intend to do this, but her argument erases the concept of “trans.” Moreover, if there’s no such thing as “trans,” then there is no such thing as “cis.” We are either boys or girls, some with vaginas and some with penises, neither exclusive to gender identity. With this argument, has Webberley committed the crime of “trans erasure”? Is she not denying the existence of trans people?
The debate also covered cross-sex hormones. The problem here follows from what was stated above. Webberley says we are merely giving the boy (which he is already, thanks to gender identity) testosterone because he does not have testes to produce it. But, according to Webberley, some boys have ovaries, which produce estrogen. So why would doctors not let him fully develop according to the trajectory of a boy with ovaries? Why work at cross-purposes with the boy’s body? The doctors aren’t fixing anything because nothing is broken. Society needs to accept him for what he is, not how he looks.
Webberley’s argument is cracked. It is entirely circular. A boy is a boy because he or others say he is, a thing that they cannot define. The truth beyond the circular is that some girls have come to believe, for whatever reason, that they are boys. It’s like a girl with anorexia who thinks she is fat. The appropriate course of action is psychological counseling to help her see herself the way she is objectively: emaciated and on a path to self-destruction. We don’t prescribe her Ozempic or perform bariatric surgery. She’s not really fat; she thinks she is. We do not affirm her delusion. That would be medical malpractice.
As for whether adults should be able to change their bodies, Keen failed to make the relevant point when this subject was raised. It is not whether a person who thinks he is a cat believes he should have the freedom to undergo surgery to make himself appear more cat-like. The ethical question is whether doctors should be able to make the delusional man more cat-like. If a man thinks he has one arm too many, we don’t amputate one of them to make him happy. He is clearly suffering from a brain or psychiatric disorder, and the ethical thing to do is deal with that, not manufacture a physical disability.
Gender affirming care, which is, in point of fact, sex-denying and not care at all, is a paradigm of medical atrocities. Doctors who commit atrocities should go to prison. Nazi doctors were hanged at Nuremberg. Helen Webberley belongs in prison.
Kellie Jay Keen
Lots of other things were said, but Webberley went full fascist at the end of the debate, saying that people like Kellie Jay Keen are not entitled to their views, nor should debates like the one they just had—that she had agreed to participate in—be allowed. What should happen to those who criticize gender identity doctrine?? Criminal prosecution, Webberley said. Only Helen Webberley’s views should be allowed. Every podcast on the topic should be a celebration of gender identity doctrine. I’m not exaggerating. She said all this and more. She even said that correctly gendering a queer person should be a crime.
Keen, for her part, agrees with me concerning atrocities. She also agrees with me on free speech. She does not advocate punishment for those who believe gender identity is a thing. One is free to say that some girls are really boys with vaginas. Others are free to criticize this belief. But those who act to harm others—that’s a different matter. Speech acts and atrocities are qualitatively different things.
A self-sealing logic is an argument system that negates all outside criticism by treating any challenge or doubt as proof that the challenger is wrong. If the claim that Zionists control US foreign policy is challenged, for example, the challenger is part of the conspiracy to perpetrate Zionist control over US foreign policy. He is more than an apologist for Zionism. He is a fellow traveler. If he denies the claim that there is a genocide in Gaza, then he is the equivalent of a holocaust denier. The genetic fallacy is at work here, as well. At the heart of the compound fallacy is the assumption that Jews orchestrate life and that anybody who rejects the assumption is part of the orchestra.
The theory that “Jews run the world” is a longstanding antisemitic claim asserting that Jews, acting as a coordinated group, control banks, corporations, governments, the media, and other major institutions to manipulate world events for their own benefit. This debunked (absurd on its face) belief has infected the worldviews of both the far-right and far-left. We see it among the Woke Reich, in the content of social media influencers such as Tucker Carlson and Candace Owens. We see it on the left in the Democratic Socialists of America. If one attempts to debunk it, which I do for the benefit of their audiences, he is dismissed as an agent of a Jewish cabal.
The compound fallacy is necessary because, as noted above, the theory has no credible evidence to support it. It relies on fabricated documents, selective anecdotes, and stereotypes. Despite having been thoroughly discredited, these claims have persisted because they offer a simple explanation for complex economic, political, and social problems. The fallacy is protective; it negates rational discernment. The cracked theory is functional, used to scapegoat Jewish communities. Scapegoating is the primitive impulse of the stupidified mind, a distraction from the real causes of human suffering. Thus it persists because it is useful for dividing and manipulating the masses. Because scapegoating is irrational, it depends on the irrational mind.
To say that antisemitism is harmful is to state the obvious. That’s the purpose of it. Antisemitism has played a significant role in justifying discrimination, pogroms, and, ultimately, the Nazi persecution and murder of millions of Jews during the Holocaust. The theory did not end with the Nazis. It is used today to undermine Israel and justify terrorism against Jewish civilians. The theory that Jews are puppetmasters pulling strings is ancient and perennial, and it has been used to divide the common folk and to obscure the reasons why things happen as they do for centuries. Just and rational minds know this, and are frustrated to see the reemergence of the ancient hatred at scale.
More recently, many decades now, the logic of this theory has been expanded to include all white people in the hatred. You’ve heard the line before, I’m sure: Whites control banks, corporations, governments, the media, and other major institutions to keep down blacks and other minorities. I show a propaganda film in class called The FBI’s War on Black America. It is told from the perspective of left-wing black activists and intellectuals working from the Black Panther perspective. I want students to experience a narrative from a particular standpoint to gain a deeper understanding of black nationalism. In the documentary, a journalist rants about the “white-owned” and “white-controlled” media. He asserts that the story of the FBI COINTELPRO operation has been warped by white supremacy—even though an almost exclusively white Congress exposed it and other clandestine operations on network television in the 1970s.
Published by Rutgers University Press
The book highlighted above, Global White Supremacy: Anti-Blackness and the University as Colonizer, by Christopher Collins and his coauthors, is one of many academic productions portraying whites in the same way antisemites portray Jews. The spread of democracy, liberal values, and reason is not the persuasion of better ideas, but the work of global white supremacy. Rutgers University Press summarizes Global White Supremacy:
“The trajectory of global White [sic] supremacy is deeply historical and contemporary—it is a global, transnational, and imperial phenomenon. White supremacy is sustained through the construction of inferiority and anti-Blackness. The context, history, and perspective offered by Collins, Newman, and Jun should serve as an introduction to the disruption of the ways in which university and academic dispositions have and continue to serve as sites of colonial and White supremacist preservation—as well as sites of resistance.”
Collins et al.’s book obscures the reality that the university and academic dispositions, captured by the left, press in the opposite direction, recoding anti-white bigotry as “resistance.” Resistance to what? To the Enlightenment and liberal values. For the enemies of freedom and republicanism, whites are the color of the West. It would be better if there were fewer of them, as Joe Biden opined (see Joe Biden and the Ultimate Source of Our Strength: “an unrelenting stream of immigration, nonstop, nonstop”). Raising the specter of “anti-blackness” is a bogeyman to distract the reader from the anti-whiteness that motivates the authors.
Published in 1994
Need another example? David Roediger’s collection of essays in Towards the Abolition of Whiteness might suffice. According to the publisher’s summary: “At a time when prevailing liberal wisdom argues for the downplaying of race in the hope of building coalitions dedicated to economic reform, Roediger wants to open, not close, debates on the privileges and miseries associated with being white. He closely examines the way in which white identities have historically prepared white Americans to accept the oppression of others, the emptiness of their own lives, and the impossibility of change.”
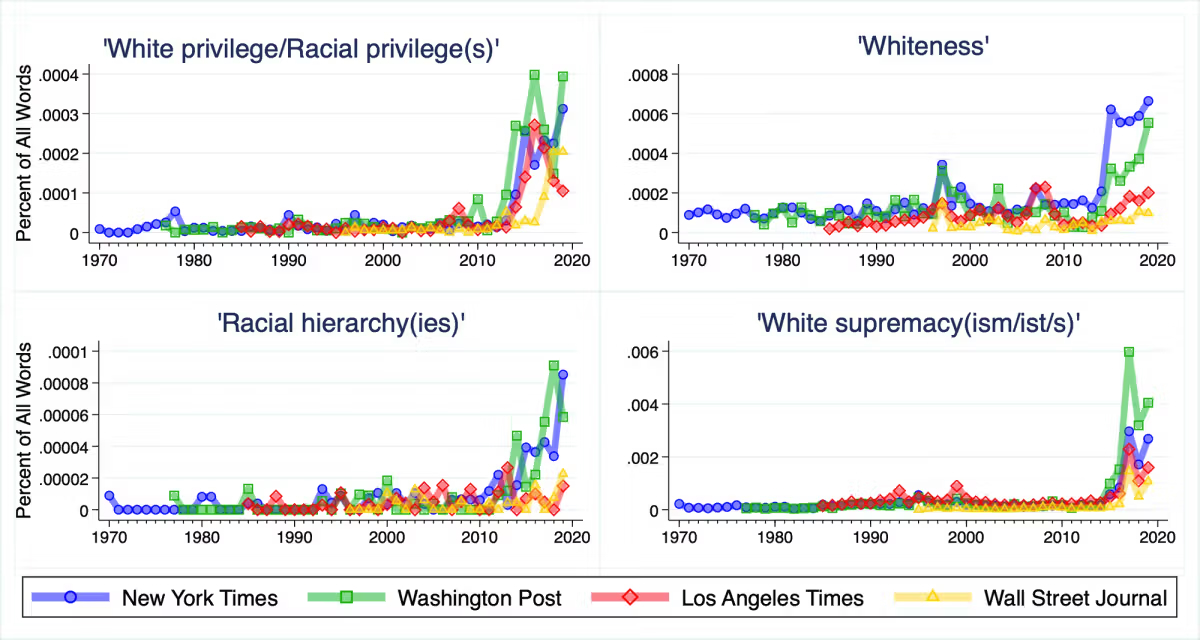
While most of us know about antisemitism, we rarely hear the parallel between antisemitism and anti-white bigotry. However, it is vital to preserving the West to recognize that the far-left weaponizes identity to advance the project of managed decline of the American Republic. Recall that, around 2010, major US magazines and newspapers flooded the zone with academic jargon, “systemic racism,” “white privilege,” and “white supremacy.” Zack Goldberg documented this in his article “How the Media Led the Great Racial Awakening,” published in Tablet in August 2020. It wasn’t long before these, and other words, became commonplace.
Some of Goldberg’s evidence
Just as disaffected Germans and the human penchant for scapegoating were marshalled for the National Socialist project, disaffected Americans, prepared by indoctrination in anti-white bigotry, are being marshalled for the woke agenda—democratic socialism, Islamization, and all the rest of it.
“Aren’t you doing the same thing, Andy?” I can hear it now. “Isn’t all that a conspiracy theory? Aren’t you scapegoating?” Not at all. Don’t be absurd. Calling out the anti-West left for its machinations is entirely unlike antisemitism. The far-left is not an ethnic group (nor is the far right that’s jumped on the antisemitic train, while, like its left-wing counterpart, cozied up to Islam). It’s an organized political force that opposes the West and promulgates anti-white rhetoric to advance its cause. It does all this openly. And it’s making strides. The Protocols of the Elders of Zion is a forgery. Global White Supremacy and Towards the Abolition of Whiteness are real books. Major magazines and newspapers, as well as cultural programming, are real developments.
The true elites and their minions announce their desires. The programming operates in the open. The results are undeniable. Western youth are being indoctrinated to hate America and Western values, and the quickest route to scrambling their minds is anti-whiteness. Elites manufacture guilt and leverage it for power. The Democratic Party—the party of transnationalism—embraces the hate. Who could forget the symbolism on display on June 8, 2020, when top congressional Democrats—including House Speaker Nancy Pelosi and Senate leader Chuck Schumer—knelt in Emancipation Hall at the US Capitol for 8 minutes and 46 seconds to honor the overdose death of career criminal George Floyd and protest police brutality. They knelt while American cities burned. They were endorsing the color revolution that anti-white bigotry fomented.
In many ways, the left today is Maoist in orientation. It is anti-family, anti-tradition, and anti-freedom. The left, bankrolled by global financiers, models Mao’s Cultural Revolution—right down to the struggle sessions. Mao Zedong launched the Cultural Revolution in 1966 to whip up revolutionary fervor, reassert his authority over the state, and eliminate capitalist, cultural, and traditional elements from Chinese society. The figurehead of the Chinese Communist Party formulated a foreign policy focused on promoting global anti-imperialist revolution, branding the United States a “paper tiger” and supporting national liberation movements in the Global South, i.e., those places lying outside the West (the Global North). This is the politics of today’s left.
There’s a reason social influencer Hasan Piker, dressed like Mao, has become the folk hero for democratic socialists. He fuses socialism and Third Worldism, in particular Islamism, in his messaging. His rhetoric is Maoist, and it finds purchase among young Americans prepared for generations to receive the message. Piker has millions of followers. One will watch his content, see a stupid man, and wonder why he is so popular. The tragic fact is that anti-white bigotry has made millions of Americans not only self-loathing but stupid.
Piker began his media career working for The Young Turks—a progressive network co-founded by his uncle, blowhard Cenk Uygur—where he hosted and produced the viral political series “The Breakdown.” The Young Turks are in many ways the mirror image of the Woke Reich—Carlson, Marjorie Taylor Greene (a Georgian politician who recently resigned from the House of Representatives), and Thomas Massie (overwhelmingly rejected by Kentucky voters in his bid for Senate reelection). On the right, the scapegoating is more exclusively Judeocentric, but the spirit is the same, and the Woke Reich is turning its back on those of European Christian descent.
The Young Turks have become explicitly and virulently antisemitic. Uygur and his sidekick Ana Kasparian post antisemitic content on X daily. They are, moreover, at the forefront of fomenting anti-white bigotry, despite being white themselves, and leaders in advancing the Islamist project. Kasparian, the child of Armenian refugees, appears to have forgotten that more than a million of her people were murdered by Ottoman Turks. The reach of TYT extends far beyond what one might suppose watching their unhinged content. Piker played a major role in Dr. Abdul El-Sayed’s victory in the Michigan Democratic Senate primary. Piker is also influential on Zohran Mamdani, the New York City mayor, a Shi’a Muslim belonging to the same religious order as the ruling class of Iran.
Social media influencer Hasan Piker discovers Mao’s Little Red Book
The woke left worldview is rooted in anti-Western postmodernism and its offspring—critical race theory, queer activism, and post-colonial studies. The organic intellectuals of Third Worldism, having insinuated themselves into the university, enjoy an endless supply of young people, already confused by the culture industry and prior education, who enter their classrooms to be indoctrinated further in anti-West and anti-white ideology. The university has become the finishing school for anti-Jewish and anti-Western activists.
The Red-Green Alliance, with wealthy financiers bankrolling street-level action, seeks the end of the modern nation-state. In its stead, they intend to entrench a global system controlled by transnational corporations. Rigid ideological systems, such as Islam, and more broadly (what is presented as) socialism, will keep the masses ignorant and passive. Key to this strategy is anti-white bigotry. Be ready for it: they portray those who call them out on it as white supremacists. That’s the trick of the self-sealing logic. The only white person worth listening to is one who self-loathes and nods along with the anti-white bigot.
* * *
We don’t need to speculate about whether the DSA is an apologist for Islamofascism. They will tell you to your face that they are. The DSA has managed to mix together Maoism and Nazism in an ideological stew that is shaping the politics of the Democratic Party. This is the most dangerous development in our lifetimes. One of the two major political parties is openly embracing antisemitic totalitarianism.
Joe Scarborough looks visibly sickened as he hears DSA co-chair Megan Romer say October 7th was "largely inevitable" and admit she "probably would have" attended a pro-Hamas rally the day after the massacre.
Joe Scarborough is right to be shocked. But is he really? He has to realise that he played a major role in this development by portraying the ordinary liberalism and conservatism of Donald Trump and MAGA as “fascism,” while downplaying the twin threats of Islam and socialism. MSNOW and other news networks prepared the ground for DSA’s madness. And the reason for this is that both the culture industry and the Democrats represent transnational corporate power. This is what they pined for. They can’t now claim to be shocked. Scarborough knows it looks bad, so he taps his pen on the table.
Look at who is sitting next to him. Do you know who that is? It’s the daughter of Zbigniew Brzezinski, the first director of the Trilateral Commission and National Security Advisor under Jimmy Carter. She knows what all this is about. Mika is Joe’s wife.
In the seventh century AD, there was a Jewish group living in and around Medina called Banu Qurayza. The archangel Gabriel appeared to Muhammad while he was bathing and asked him why he rested while Allah’s enemies remained nearby. Gabriel directed Muhammad to take up arms against the Qurayza.
Seizure of the Banū Qurayza stronghold. Illustration from Ḥamlah-i Ḥaydarī, by Muhammad Rafi’ Bāzil
Muhammad’s forces besieged Banu Qurayza until the Jews surrendered. The men were beheaded in Medina’s market, and the rest were distributed as captives and made slaves. With the earlier expulsions of the Banu Qaynuqa and Banu Nadir, no Jewish community remained in Medina after Muhammad was done. Medina had been ethnically cleansed of Jews.
We are told that a small minority of Muslims are Islamic extremists. Yet their own prophet was an extremist. Muslims are told that Muhammad was a model man, and Muslims are to emulate him. “What would Muhammad do?” is a radically different question than “What would Jesus do?” Muhammad was not a benevolent prophet who brought love and peace for mankind. He was a genocidal megalomaniac who enslaved, killed, and maimed men and babies, and raped women. In truth, there is no difference between Islam and Hamas. Hamas is not an aberration in Islam. Hamas is Islam. (Here is where I disagree with Ed Husain. See The Final Solution: The Globalist Ideology of the Muslim Brotherhood.)
We’re told that Islam means “peace.” But the peace Muslims seek is achieved by eliminating all non-Muslims. Yet even that doesn’t bring peace. Muslims kill each other. What Islam literally means is “submission” or “surrender.” To whom is the world supposed to surrender? Muslims tell us: submit to the will of Allah. But who speaks for Allah? Muslim clerics and terrorists. Therefore, what Islam really means is submission to the will of Muslims. If one doesn’t submit to Muslims, then one is beheaded or enslaved. The Muslim may offer conversion, but that is itself a form of enslavement.
For those who wish to insist on distinguishing between Hamas and Gazans, I will remind them that history records that ordinary Germans enabled the Holocaust (See Daniel Goldhagen’s 1997 Hitler’s Willing Executioners: Ordinary Germans and the Holocaust). The Judeocide was a collective effort. To be sure, there were Germans who did not wish to see this happen, but it did not matter. They were in the minority. And they were afraid. Eliminationist antisemitism gripped enough Germans to make genocide possible. There are no good Germans in an antisemitic mob. One cannot be a good person and be an antisemite. For this reason, widespread antisemitism in Islam condemns the ideology.
The only way to deal with those hellbent on exterminating people-groups is to defeat them and deprogram the population. Deprogramming is not pretty, but it’s necessary. In the aftermath of WWII, the German population was de-Nazified. That meant eliminating the Nazi Party and its organizations, removing committed Nazis from positions of influence, punishing major offenders, and changing German institutions so that they could support a democratic society. Nazi property was confiscated. Nazi propaganda and symbols were prohibited. Nazi monuments, signs, street names, and other public manifestations were removed.
Denazification applied to education, finance, government, industry, the press, and other institutions. A university professor who had been an enthusiastic Nazi, a civil servant who had advanced through the Party, a schoolteacher who had been an active Nazi propagandist, or an industrialist who had substantially supported the regime—all could potentially be removed from his or her position. Some of the measures are uncomfortable from a free speech standpoint, to be sure, but then there is no greater threat to free speech than Nazis and Islamists.
What is required in Gaza is the elimination of Hamas and the de-Islamification of the Gazan population. This requires, as it did in Germany, the occupation of Gaza until the population is deprogrammed. Israel need not eliminate the Arabs residing there (but if they want to leave, then they should be encouraged to). More than twenty percent of the Israeli population is Arab Muslims. Self-evidently, Israel has no desire to eliminate Arabs. De-Nazification did not mean eliminating the Germans as a people. What de-Islamification does mean is eliminating an authoritarian and genocidal movement in the same way the West eliminated the Nazi state and suppressed National Socialism.
Some will say that eliminating Islam is no different than the elimination of Jews in Medina under Muhammad. If it was wrong for Muhammad to conquer the Qurayza and erase Judaism in Medina, the argument goes, then it is wrong for Israel to conquer Gaza and erase Islam in Medina. But the equivalency requires Jews and Muslims to exist on the same moral plane. To suggest they do is to claim that Jews and Nazis exist on the same moral plane. Such a claim is absurd on its face. Moreover, Jews are a people-group. Islam is an ideology, not a people. Islam is no more a people than Nazis were a people. Liberating Germans from National Socialism was the task of moral people. And so it is the task today to liberate Arabs from Islam.
* * *
The Internet is rife with attempts to apply the Golden Rule to morally asymmetrical groups. “Israel has nuclear weapons, so why can’t Iran have them?” Because Israel and Iran are not the same. You must hate the Jews and love totalitarianism to not see that. Israel is a liberal democracy. Iran is an authoritarian state. Israel wishes only to protect its citizens. Iran and its proxies—Hamas, Hezbollah—strive to eliminate Israel. When called to military action, Israel wages defensive war, carefully avoiding civilian casualties. Iran wages aggressive war to bring about an Islamic world order and kills everybody who gets in the way. And when they aren’t killing people, they’re frightening them into silence—or conscripting the disaffected into their ranks.
The defenders of Islam do the same thing in debates about the Qur’an. It has become predictable in these debates to say, “What about the Torah? There are horrors in there.” Indeed, there are. The ancient Hebrews of three thousand years ago were like their neighbors. They were tribal. Kill or be killed was the way of the world. Conquest, slavery, and genocide were normal in ancient times. But the modern Jew is not the ancient Hebrew. He kills not for conquest but in self-preservation.
We cannot say the same for the modern Muslim. The horrors of October 7, 2023, testify to the grim reality that Muslims today are of the same character as those who eliminated the Banu Qurayza, beheading Jewish men and raping Jewish women. Muslims have not changed. And they won’t change because, unlike the Judeo-Christian tradition, Islam is intrinsically totalitarian.
Jews did not wish to convert others to Judaism. Christians no longer spread the Gospel by the sword but by persuasion. Indeed, we rightly condemn those periods when Christians behaved otherwise. We condemn forced conversion because we in the West are allowed to criticize faith. Criticizing Islam is risky business. Muslims will claim there is no compulsion in Islam, but those who have been forced into it beg to differ.
* * *
Having agreed that the Torah documents atrocities, how does that make the Qur’an okay? Is it okay for Bob to kill Tom because Bill killed Tim? Stalin and Mao killed millions. Does that make Hitler less evil?
In my thirty years of teaching, during my lectures on authoritarianism, I have on more than one occasion had a student bring up Stalin in the context of my account of the Nazis’ killing operations. I will get to Stalin, I assure the student, but why raise the matter of Soviet Communism now? I am suspicious that the student is an apologist for Hitler—or supposes without any evidence that I’m an apologist for Stalin. Charitably, I don’t make my suspicions explicit, but I am suspicious, nonetheless.
Flip the scenario. Suppose I was talking about the atrocities perpetrated by Stalin and a student reminds the class that Hitler also committed atrocities. As we can see from the stickers on his laptop, he is a socialist. Is he downplaying Stalin’s crime because Hitler was also a criminal? An objective account of the Soviet Union makes socialism rather unattractive, after all. It is reasonable to suppose that the socialist student is trying to hold on to his faith. His invocation of Hitler is a deflection. “What about Hitler?” should also always be met with suspicion.
Wrongdoing by others does not negate wrongdoing. Your son’s bad behavior is not excused because others’ sons behave badly. If it was wrong for Moses to have commanded the Israelis to kill all the Midianite men, women, and children save the virgin females, then it was wrong for Muhammad to perpetrate atrocities in Medina. Here, we can identify a moral equivalency. The Golden Rule applies. It falls to Muslims to hold up their end of the rule. They will always fail to do so.
It is not the purpose of the defenders of Islam to find moral equivalency. The purpose of raising the Torah is to deflect from the Qur’an and the evil deeds of Muhammad. At the heart of deflection is the defense of Islam. Those who warn about Islam are portrayed as hypocrites for defending Western Civilization from the barbarian. Noticing the drastic rise of rape in several European states that accompanies Islamic migration to the region is met with charges of bigotry. The defenders of the West are “Islamophobic” for finding in Islam a warrant for rape and genocide. But a phobia is an irrational fear and loathing. There are still rational men in the West. And there remains uncorrupted instinct (see The Bad-Smell Ant: Disordering a Nation’s Protective Instinct).
“There are some ideas so absurd that only an intellectual could believe them.” — George Orwell
In 2024, during a faculty meeting, one of the faculty members (now teaching somewhere else) deemed me a “heterodox.” Oh horror, I thought; I stand accused of heterodoxy. For context, this was during the petition drive organized by the Green Bay queer lobby to demand the university fire me for the disagreeable things I write on Freedom and Reason (see The Snitchy Dolls Return).
To clarify, a heterodox is somebody who dissents from the orthodoxy, i.e., the consensus opinion. The faculty member was informing me that my ideas stand outside the mainstream. It was an interesting take, since my views on the pressing issues of the day—criminal justice, child protection, equality, gender, immigration, women’s rights, and so forth—are orthodox from the standpoint of the general population.
As it turns out, I am rather mainstream. Indeed, at many points, when viewed from the outside, it is the university orthodoxy that is in fact the heterodox orientation. This is especially true not only of the humanities and the social sciences, but of administrative logic, with DEI programming and all the rest of it. The university has lost prestige—like Hollywood and the mainstream media—because the image of America it pumps out does not resemble the America normal people desire.
Most Americans believe that individuals should be judged on merit and not the color of their skin. They believe in borders and immigration law and enforcement, that the police and prisons play a vital role in public safety, that women should have exclusive spaces so men don’t overpower them, that children should be protected from sexualization, and that gender is binary and immutable. Most people will tell an academic that a woman is an adult female human, and roll their eyes when he condescends to tell them that “It’s complicated.” The academic is thinking most people are stuck in the past.
The common folk believes these things not because they are not well-educated (many of them are, in fact), but because the facts align with common sense, and the average man knows this intuitively. Most Americans have a sense of fair play (“equity” to be fancy with words). They are not going to indulge in overly complex theories, i.e., rationalizations, that attempt to explain away facts that are self-evident to them. Nor will they accept that their native understanding of justice is misguided. Because it’s not.
To presume that the opinions of the professoriate represent the orthodoxy is to announce that one lives inside a bubble where the academy is the universe, tightly circumscribed by the special laws of relativity our betters crafted with dense and verbose language—as if the space they inhabit is an island all to itself, where the islanders are free to create an alternate reality by speaking in tongues. That island has strong borders, by the way, and they are well policed.
Paradoxically, they have devised an interesting rule that makes it difficult to vote dissenters off the island: the institution of tenure. Still, the island can make it difficult for the dissident. In Japan, management uses passive-aggressive isolation tactics to encourage employees to voluntarily leave their positions. Strict Japanese labor precedents make direct termination for employees extremely difficult, prompting some firms to use gray-area tactics to bypass severance. There is a version of this on the island. The institution has ways of ostracizing and demoralizing dissidents. Colleagues a man has known for years turn cold, even when they had a social life together. There is no “university community.” It is a bureaucracy.
Because man is a social animal, passive-aggressive isolation takes its toll. In the case of the university, it is particularly demoralizing because—one would think— professional thinkers come together in one place to challenge orthodoxy. Critiquing belief systems is an endeavor that requires robust pursuit of the dialectic and the freedom to publish and speak without consequences. This becomes effectively impossible when ideology is elevated above reason and science. Academic freedom can be upended in a myriad ways short of blatant censorship.
It used to irk me a bit when people would say, “Those who do, do; those who can’t, teach.” I am no longer irked. It’s a truism that finds me searching out any elitism that may be lurking in my head and exterminating it. I have certain skills to be sure, and they benefit society as long as I keep them from ideological corruption, but my talents don’t make me better than anybody else. Most academics I know do not share this value. Decades inside the bubble have left no doubt about this. They think themselves the betters of the common man. And they generally hate the doers, even when their actions serve the interests of the worst among them.
I teach, and I love it. That academic associations, curricula, disciplines, and all the rest of it should keep me in a box—that I do not love. I never sought priesthood, and the cloistered milieu of the university is much like that, and it has been stifling. I have kept my integrity, though. On the island, I am a heterodox. But there’s a boat waiting on the shore.
Every time there’s a mass shooting, progressives hold their breath, praying that it won’t be another Muslim or queer person. Every act of Muslim or trans terrorism punctuates their ongoing denial about the problem of these movements. The left confirms its awareness of the danger these ideologies present to public safety when the shooter is neither one of those types. When it’s a white man, presumably Christian, they call out “MAGA types” for their alleged silence. Yet, it’s the double standard on their side that proves the progressives are disingenuous—and confirms their penchant for projection.
News story of shooting
The shooter in the latest high-profile mass shooting was a white man named Chad Williams. Armed with an AR-15-style rifle, the 24-year-old killed three people and wounded several others at an In-N-Out Burger in Twin Falls, Idaho, before taking his own life. Williams ended the nightmare after an armed civilian, Jordan Salinas, used his FN Five-seveN semi-automatic pistol to disrupt his plans.
The incident recalls another shooting, this one in Boise, Idaho, by Jacob Bergquist, a 27-year-old white male. Bergquist was a white supremacist. White supremacy suggests Bergquist’s motives. We’re still waiting to learn more about Williams’ politics, but the fact that he is white cannot explain the fact that he killed three people. We need to know what Williams believed.
He’s not Muslim. He’s Christian. He’s not brown. He’s white. He’s also pro-Israel.
There are two major problems with the obvious attempt to make conservatives appear racist and transphobic by leveling the charge of hypocrisy. Firstly, race tells us very little, if anything, about motive. Would not those defending their tribes agree? You’d think so, but you would be wrong. When the shooter is white, a category they narrowly circumscribe to mean right-wing Christian, his motive is his whiteness.
But this raises a problem for progressives. For, secondly, Muslim is not a race. The posts rationalize grouped variation in mass shootings by comparing white and Muslim as if they’re the same category of thing. The 9-11 hijackers were white men. They were not some other race because they were Muslim. Did their whiteness fly planes into buildings? No. They brought down those towers because they were Muslims. For the woke, America deserved it. It was a case of chickens coming home to roost.
Moreover, most trans shooters are white males. However, white men escape the wrath of woke zealots by declaring themselves to be women. Queer identity erases not only their maleness, but also their whiteness. Queer is the act of stepping into oppression. The man the transwoman was (and still is) is dead. Once a man identifies with an oppressed group, his acts of violence are transformed into justice or blamed on the oppressor.
Race is a category based on physical appearance. One is not white because he believes he is. White is not an ideology. If the Twin Falls shooter had been a Muslim or trans person, then it would be reasonable to ascribe motive, since Islam and gender identity are ideologies. One may be wrong to attribute motive to ideology. Not every Muslim kills for Islam. But it’s a fair assumption. If it turns out that Williams was a white supremacist like Bergquist, then that might suggest a motive, but we don’t have enough information yet. That he is neither Muslim nor queer is enough for woke types to flood X with charges of hypocrisy.
It is worth keeping in mind that, of the 440 million Muslims living in the Middle East and North Africa, the vast majority of them are white. Europe is home to 46 million Muslims—majority white. There are another 25 million Muslims in Albania, Bosnia and Herzegovina, Bulgaria, Kosovo, North Macedonia, Russia, and Serbia. Their race? You guessed it: for the most part, white. Many Muslims in the Western Hemisphere are white. Does whiteness explain Muslim terrorism? Or does Islam? Progressives get around the problem by reracializing Arabs.
If the shooter is a far-right terrorist, I will condemn it. But I already condemn it. I condemn mass murder whether the man is a white supremacist or a Muslim. Readers of this platform know that I spent a great deal of time raising awareness about patterns of gun violence and debunking political distortions surrounding it, such as the claim that most mass shooters are young right-wing white males.
It’s enough for me that Williams killed several random people to draw my condemnation. But I’m not like the woke leftist. I can and do condemn gun violence on all sides. The progressive only condemns violence when it is perpetrated by Christian white cismen. When the violence is coming from inside the house, his silence is deafening.
Production note: I obtained the transcript of Ed Husain’s remarks on Triggernometry from YouTube, fed it into ChatGPT, and asked the bot to remove timestamps and reproduce the conversation in a coherent form. I then produced a summary of the output, focusing on Husain’s observations that were pertinent to the analysis presented here. I’ve been careful to ensure that the reader can differentiate between Husain’s ideas and my own, which are highly similar.
To put my purpose in doing this straightforwardly, I am using Husain’s narrative to reinforce my own analysis for the reader and to introduce Husain to those who may be unfamiliar with his work. Although I have some disagreements with Husain (which will emerge over the course of the analysis), he is in the main correct about the history of the Muslim Brotherhood and its implications.
Ed Husain is a British writer, academic, and political adviser best known for his work on Islamism, radicalization, the Middle East, and relations between Islam and the West. He teaches at Georgetown University and Columbia University. Last month, he appeared on Triggernometry to discuss the problem of Islamism and the Muslims Brotherhood. In this essay, I summarize his argument for readers to use in explaining the problem to others. What Husain makes clear, in my view, is that Islamism is the modern-day instantiation of National Socialism. It is not only like Nazism ideologically, but, as I have shown in previous essays, historically allied with Hitler and his project to exterminate world Jewry.
For Husain, the Muslim Brotherhood should be understood primarily as an ideology rather than simply an organization. Although the Brotherhood possesses formal institutions and affiliated groups, its true significance lies in the political worldview it introduced into modern Islam, which in turn shapes Muslim thought. Rather than representing the continuation of a long-standing Islamic tradition, the Brotherhood represents a decisive break from classical Islamic thought. While I disagree with Husain about the distinction between Islam and Islamism (they are closer than he thinks), there is much merit in his argument, especially in the practical sense in that it allows moderate Muslim leaders to sway the masses towards a reformist path.
Founded in Egypt in 1928 by Hassan al-Banna, the Muslim Brotherhood emerged as a modern revolutionary movement whose ambition was to establish an Islamic state, restore the caliphate, and ultimately replace the nation-state with a transnational political order governed by its own interpretation of Islamic law. In Husain’s view, this ideology later became the intellectual foundation for organizations such as Hamas, al-Qaeda, and ISIS, while also shaping Islamist activism throughout the West. The Red-Green Alliance we see in the United States is rooted in the Brotherhood’s ideology. These are the politics behind the Council on American-Islamic Relations, or CAIR. The Brotherhood’s ideology is what motivates the Islamization of the West, including the corruption of Western academia.
The origins of the Muslim Brotherhood lie in three grievances articulated by its founder, Hassan al-Banna. First, al-Banna regarded the abolition of the Ottoman Caliphate in 1924 as a catastrophe for the Muslim world. The disappearance of the caliphate symbolized the loss of Muslim political unity and global influence. Al-Banna believed that Muslims required a single political authority capable of confronting Western powers and resisting competing civilizations. The Brotherhood’s ambitions are totalitarian.
Second, al-Banna objected to the growing presence of Western missionaries, particularly American evangelical organizations operating throughout Egypt. To him, their activities demonstrated not merely foreign religious influence but Muslim weakness and political decline. The reader must remember that, while Muslim teaching claims the Abrahamic god and accepts Jesus as a prophet in Islam, Islam rejects the divinity of Jesus. They must diminish Jesus to clear the way for Muhammad to be the last prophet of God’s message. The diminution of Christ is essential for establishing Islam as the final solution. Once this view is accepted, the Abrahamic faith and its history become fully Islamized, and any rejection of it makes the heretic the proper subject of subjection and violence.
Third, al-Banna viewed the Westernization of Egyptian society as evidence of cultural decay. This mirrors the way German National Socialism depicted the Jews as responsible for Entartung or degeneracy. The cosmopolitan life of Cairo—with its alcohol consumption, dancing, European fashions, and expanding liberal culture—appeared to al-Banna as a surrender of Islamic civilization to Western values.
These three developments convinced al-Banna that the Muslim world faced a comprehensive civilizational crisis requiring political action rather than simply religious renewal. For Husain, Islam is a religious system, like any other (Thomas Jefferson viewed Islam similarly). The problem of Islamism lies with the politicization of the Muslim faith and the fusion of religion and state. In my view, Islam is a political system, which the imposition of Sharia makes clear. But conceptualizing Islam as a religious system makes it (potentially) reformable. From a pragmatic standpoint, characterizing it as such may have utility.
Hassan al-Banna
Al-Banna first sought support from Egypt’s established religious authorities. He appealed to Al-Azhar, the most prestigious Sunni institution in the Muslim world, urging it to confront these developments. According to Husain, Al-Azhar rejected his revolutionary urgency, preferring gradual scholarship and religious guidance over political mobilization. Al-Banna then approached Egypt’s Sufi orders, hoping they would embrace his vision. But they also rejected him, insisting that spiritual reform begins with the individual rather than political confrontation. They viewed his activism as dangerously politicized and inconsistent with the prophetic model.
These rejections proved decisive. Husain argues that this moment marked the Brotherhood’s fundamental departure from mainstream Islam. Instead of accepting the accumulated authority of classical institutions, al-Banna created an independent ideological project centered on capturing political power. In a world where secularism resists the pull of religious zealotry, capturing political power requires force. Thus, in places where the project embeds, those advocating its goals have eventually turned to terrorism and other forms of political violence.
It is crucial to note that, while the US government has not designated the entire global Muslim Brotherhood as a foreign terrorist organization (FTO), it has officially designated specific chapters and branches as terrorist entities. That’s a start, but the government has met resistance all along the way. Experts have warned the Trump Administration against designating the Brotherhood as a whole an FTO. The reason why we will come to that in time. It suffices to say here that their reasoning is not sound. The only way to deal with terrorism is to recognize it and disable it—and that means going to the heart of the problem: its ideology. (This is true of Antifa, as well.)
* * *
Husain argues that the Brotherhood should be understood less as a religious revival than as a modern political ideology. Its central objective became the creation of an Islamic state governed by Sharia as state law. Unlike the modern nation-state, however, this state would possess no permanent borders. It would exist as an expanding political entity—a caliphate—with frontiers rather than fixed territorial limits. Its mission would ultimately be universal rather than national.
This vision, which aligns with the spirit of National Socialism, fundamentally rejects the legitimacy of sovereign nation-states. Whereas the modern international order is built upon independent states operating within recognized borders and legal jurisdictions, the Brotherhood regards such arrangements as temporary historical accidents destined to disappear beneath a unified Islamic political order. Islamists must Islamize the countries in which they embed. Hitler viewed the nation-state in the same way. He disregarded boundaries and Nazified the territories he conquered.
For Husain, this ambition distinguishes the Brotherhood from traditional Islamic scholarship. Classical Islamic literature, he contends, contains no systematic doctrine requiring Muslims to establish a single global Islamic state. Throughout Islamic history, multiple Muslim governments existed simultaneously, often independently of one another. Even during the lifetime of the Prophet Muhammad, Muslim communities lived under different political arrangements. Consequently, Husain argues that the Brotherhood’s doctrine of a universal Islamic state is a twentieth-century political innovation rather than a continuation of classical Islamic teaching.
* * *
Sayyid Qutb
While Hassan al-Banna founded the movement, Sayyid Qutb transformed it into a revolutionary ideology. Sayyid Qutb traveled to the United States during the late 1940s and spent some time there. Sent by the Egyptian Ministry of Education to study American educational systems, he spent several months studying at the University of Northern Colorado (then Colorado State College of Education).
Qutb’s experiences in the US profoundly shaped his worldview. Rather than admiring American society, he returned to North Africa convinced that Western civilization represented moral corruption. He condemned American sexual freedom, criticized women’s public independence, rejected aspects of American popular culture, and developed an intense hostility toward what he regarded as Western decadence.
After returning to Egypt, Qutb was imprisoned by the Egyptian government. His imprisonment convinced him that even governments claiming to be Muslim had abandoned authentic Islam. Popular images of Qutb often depict him standing behind bars (we saw this with the Nelson Mandela cult of personality, a strategy of generating popular support not only for the African National Conference but also the goals of the South African Communist Party). From this experience emerged one of the Brotherhood’s most influential concepts: that contemporary Muslim societies themselves had fallen into a condition of ignorance comparable to pre-Islamic paganism.
This conviction found its fullest expression in Qutb’s 1964 Milestones. In that work, Qutb argued that existing Muslim governments no longer possessed genuine Islamic legitimacy. Through the doctrine of takfir (an Islamic term that denotes the excommunication of one Muslim by another, whereby a self-professed Muslim is declared an apostate or an unbeliever), he declared that rulers—and eventually entire societies—could be regarded as outside Islam. Violence against such governments therefore became religiously justified.
According to Husain, Milestones represented a decisive transformation in Islamic thought. Earlier conservative Islamist teachings focused on resisting foreign domination. Qutb redirected revolutionary violence toward Muslim governments themselves. From this point onward, ordinary Muslims became the principal victims of Islamist violence because they refused to embrace the Brotherhood’s revolutionary program.
This piece is often missed by Western observers. To be sure, Westerners are frequently targeted by Islamic terrorists. But most political violence is perpetrated by Muslims against other Muslims. Hitler had no qualms about perpetrating violence against fellow Germans whom he viewed as deviating from the path laid before them.
Despite remaining a minority movement, the Brotherhood achieved remarkable influence. It offered simple political answers to complex problems. Its slogans condensed its ideology into memorable formulas: “The Qur’an is our constitution,” “Jihad is our path,” “Martyrdom is our highest aspiration,” and, most significantly, “Islam is the solution.”
For Husain, these slogans represent political innovations rather than classical Islamic teachings. They transform Islam from a faith concerned with worship, ethics, and spiritual life into a comprehensive political program claiming to solve every social and political problem. Followers of Christopher Hitchens know that he often appealed to the slogan “Islam is the solution” as a reason for fearing the encroachment of Islam into Western societies.
At the same time, the Brotherhood reframes political conflicts as exclusively religious struggles. Geopolitical disputes become attacks upon Islam itself. For example, the Brotherhood frequently deploys the term “Islamophobia” to convey this paranoia, as if resistance to Sharia is akin to anti-gay prejudice.
Progressive Westerners are all too eager to take up the Brotherhood’s cause. Indeed, one can trace the origins of the term to the Runnymede Trust’s Commission on British Muslims and Islamophobia’s Islamophobia: A Challenge for Us All, published in 1997. In the report, Islamophobia is defined as “an outlook or world-view involving an unfounded dread and dislike of Muslims, which results in practices of exclusion and discrimination.” Its authors assert that “anti-Muslim prejudice has grown so considerably and so rapidly in recent years that a new item in the vocabulary is needed.”
Runnymede’s intervention dovetails with the propaganda project of the Organization of Islamic Cooperation (OIC), comprised of 56 Islamic nations. The OIC pushes the UN to criminalize Islamophobia to establish in international law the criticism of a particular religion as a thought crime. The UN has acquiesced. For example, the UN Human Rights Council OHCHR on Freedom of Religion continually urges countries to implement measures against “hate speech.” While the OIC’s official positions are, at least ostensibly, antagonistic to the Muslim Brotherhood, it is no accident that both the OCI and the Brotherhood are keen on establishing Islamophobia as a hate crime.
There are considerable efforts to deny the Brotherhood’s role in creating the propaganda term. Philosopher Roger Scruton was dismissed from a government role as the UK’s unpaid housing adviser in 2019 after making this assertion in an interview published by The New Statesman in April 2019. The Spectator later published full transcripts showing selective context, and The New Statesman issued an apology for unfair representation. The British government followed with an apology and reappointed him later that year, but the episode spoke volumes about the role the charge of Islamophobia plays in silencing voices. What motivated The New Statesman’s hit piece? Islamophilia is the obvious answer. Scruton died the following year.
Whatever its origins, the term’s function is clear. Muslims are encouraged to interpret conflicts in Kashmir, Palestine, or elsewhere primarily as evidence of a global assault upon their religious identity. Once problems are defined in this manner, the Brotherhood is enabled to present its political program as the only adequate response to those it has portrayed as the enemies of Islam.
The Brotherhood’s success therefore lies not in representing most Muslims but in functioning as an organized ideological minority capable of mobilizing populations through emotionally compelling narratives centered on grievance, identity, and political redemption. However antagonistic the OIC may be to the Brotherhood, the common attitude unites them in a convergence of sentiment.
* * *
Returning to the historical narrative, following repression in Egypt during the 1950s and 1960s, Brotherhood activists dispersed throughout the Middle East. Many settled in Saudi Arabia and other Gulf states, where they entered educational institutions and influenced new generations of students. Husain notes that Qutb’s brother, Muhammad Qutb, played a particularly important role in transmitting Brotherhood ideology to figures such as Osama bin Laden.
Brotherhood members increasingly entered universities in Britain and the United States, as well, as political refugees. Rather than abandoning their ideology, they established charities, community organizations, educational institutions, mosques, and Islamic centers that gradually disseminated Brotherhood ideas within Western Muslim communities—and beyond. This is the Islamization project.
Husain presents Hamas as a model of this pattern. Beginning as a charitable and educational movement in Gaza, it gradually constructed extensive social networks before eventually developing an armed wing, which has become a proxy for the Islamic Republic of Iran’s war on the West. Thus, for Husain, charitable activity functions not merely as humanitarian work but also as the foundation upon which broader ideological and political movements are built.
* * *
A central component of Husain’s argument is that the Muslim Brotherhood should be understood within the broader intellectual context of twentieth-century totalitarian ideologies. He argues that the movement absorbed ideas circulating during the interwar period rather than simply reviving classical Islam. Like fascist and totalitarian movements, Islamism seeks comprehensive political transformation through a single ideological system. It envisions history as a struggle between true believers and corrupt societies. Rejecting political pluralism, it aspires to create an all-encompassing political order.
Crucially, the similarities are ideological rather than merely historical. Both Nazism and the Brotherhood are atavistic and globalist in character. They seek expansive political orders transcending existing borders. Both claim to possess a comprehensive solution capable of restoring historical greatness.
The Brotherhood’s slogan “Islam is the solution” reflects the same totalizing political impulse characteristic of twentieth-century totalitarian ideologies. As the co-host of Triggernometry, Francis Foster noted, it resembles the name of the Nazi project to exterminate the Jews: “the Final Solution.” Husain immediately agreed and praised Foster for so cleanly articulating the parallel.
According to Husain, Western governments have consistently misunderstood the nature of the Brotherhood. Because it often presents itself through charities, educational institutions, advocacy groups, and religious organizations, Western officials frequently interpret it as a moderate religious movement or a legitimate civil society actor. This mistakes tactical moderation for ideological moderation.
He further contends that British intelligence agencies historically tolerated Brotherhood networks because they believed these organizations could provide strategic leverage against governments in the Middle East. What appeared to be manageable political assets gradually evolved into influential ideological networks capable of radicalizing successive generations of British Muslims. The result, Husain argues, is that Western governments now confront a movement they helped accommodate while ignoring repeated warnings from Muslim-majority governments that had already experienced the Brotherhood’s methods firsthand.
Perhaps Husain’s most important—and objectionable—distinction is between Islam as a religion and Islamism as a political ideology. He insists that the Brotherhood does not represent Islam itself. Most Muslims reject its revolutionary program, just as many of its earliest critics came from within Islamic scholarship. The Brotherhood’s greatest opponents have often been ordinary Muslims and Muslim governments rather than Western societies.
For Husain, the central mistake made in contemporary political discussion is the failure to distinguish between a fourteen-century-old religious tradition and a modern ideological movement that appropriates Islamic language while fundamentally transforming its political meaning. Again, I do not agree that it is simply a matter of distinguishing between Islam and Islamism. Islamism is the fruit of Islam, but if the distinction is taken to heart by the Muslim majority and Islam can be nudged towards reform, it should undermine the more extremist versions of the religion by moderating Islamic doctrine.
I will have more to say about whether it is possible to separate Islamism from Islam (I don’t think it is). But for now, it is vital—for those serious about confronting the problem of Muslims in the West—to take Ayaan Hirshi Ali’s argument on this subject into consideration. She argues that reforming Islam itself will undercut extremism. The idea here is that Muslims should be less inclined to follow their prophet, since uncritical devotion is one of the ways extremists garner popular support.
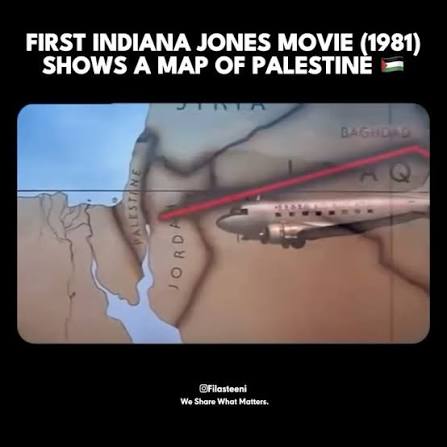
After the Romans redesignated Judea as “Syria Palaestina” in 135 AD, “Palestine” remained a geographic designation used by various empires and mapmakers for the next 1,700 years. The dramaturgist associated with the first Indiana Jones film rightly identifies Palestine on the map antisemites like to share in memes. But it doesn’t mean what they think or say it means.
Typical example of the Indiana Jones meme
The fact is that there has never been a sovereign and independent state called “Palestine.” The name designates a territory. Before the establishment of the State of Israel in 1948, Jews living there were known as “Palestinians.” The Jerusalem Post, a prominent Israeli newspaper, was founded by Jews as The Palestine Post. It was never an Arab newspaper.
There are many examples like this. The Israel Philharmonic Orchestra, a Jewish orchestra, was founded as the Palestine Symphony Orchestra. Jewish athletes competed internationally as Palestinians. There are manhole covers that carry the name “Palestine” (antisemites like to share memes of those, too).
Manhole cover in the Israeli district of Haifa
The old maps designate a location on the globe where Jews have continually existed for several thousand years. If you have a map that calls this territory “Palestine,” then your map is out of date. The old map only proves that Jews were once known as Palestinians.
When the State of Israel came into existence in 1948, it included among its citizens Jews, Arabs, Christians, Druze, and other ethnicities and religious groups. Israel is a religiously pluralistic multiethnic state—like the United States. Members of those groups became Israeli citizens. An Arab Muslim or a Jew living in Israel who would have been known as a Palestinian before 1948 is today known as an Israeli.
Arab Muslims opposed to the state of Israel came to be associated with the name “Palestinian,” especially after the Arab-Israeli War (which the Arabs initiated and suffered a humiliating defeat for their aggression) and the rise of the Palestine Liberation Organization (PLO), as a political strategy. They retain the name to clothe themselves in false legitimacy. But they are no more Palestinian than Jews are.
* * *
Rarely is it emphasized that the establishment of the State of Israel occurred amid nation-state formation across the region. Many Middle Eastern states became independent nation-states in the period after World War I, and several others gained full sovereignty or took their modern form after World War II.
We’re led to assume that Iraq, Saudi Arabia, Jordan, and others have been sovereign nation-states for centuries. But Iraq, for example, only became an independent nation-state in 1932. That same year, Saudi Arabia was founded. Other Arab states were established later. Lebanon became a state in 1943. Syria became a state in 1946. Jordan was established in 1946 as Transjordan. It changed its name to Jordan in 1949.
Many others fit the pattern. Kuwait, the United Arab Emirates, Qatar, Bahrain, and other Gulf states—they all became modern sovereign states in the twentieth century. In other words, the formation of Israel in 1948 was part of a trend of national independence in the region. Independent of ideology, there is nothing unique about the Israeli case.
So why the furor over Israel? Is it not obvious? All of those other states are majority Arab and Muslim states. Israel is the only Jewish-majority state in the region. Nobody questions the sovereignty of the Arab states. They rarely criticize the fact that some of them are monarchies and Islamic. They only question the legitimacy of Israel. Arab nationalism is accepted, while Jewish nationalism, i.e., Zionism, is condemned. The difference is the fact that the majority of Israelis are Jews and that Israel is a Jewish nation. It follows that anti-Zionism is antisemitism.
The Jews were Palestinians—just as they were Judeans before Rome renamed Judea “Palestine.” Jewish Palestinians changed the name of their homeland to Israel with the establishment of the modern nation-state. They could have named their state “Palestine,” but instead chose “Israel.” They won the right to name their state anything they wished by successfully asserting their rights to self-determination and defensive war.
* * *
If it were true that Israel is carrying out a genocide or engaged in ethnic cleansing, then there would be few or no Arabs in Israel. Yet over 20 percent of Israelis are Arab. They are citizens or permanent residents with full access to the same rights as other Israelis.
Before October 2023 (when Gazans invaded Israel and massacred Jewish civilians), approximately 150,000 Arabs from Gaza and the West Bank held official permits or crossed to work in Israel daily, primarily employed in construction, agriculture, and manufacturing. Israel was only recently forced to impose restrictions for security reasons.
There is no genocide in Israel, which, until 1948 with the founding of Israel, was called Palestine (for 1700 years). As I show in today’s article, Jews were known as Palestinians until the State of Israel was established. The genocide rhetoric is absurd on its face.
Why does this rhetoric persist? The genocide rhetoric is part of a propaganda project to delegitimize the existence of the State of Israel. Why would anybody want to do that? Antisemitism. Antisemites seek the elimination of Jews from the territory. That is what is meant by the slogan “From the River to the Sea.” There’s a word for that. Want to hazard a guess as to what that word is?
* * *
Arabs are white, and Jews are the OG Palestinians. These facts blow up the entire white settler colonizer argument. How can a people colonize their own land? Once you see the truth of the matter, the question then turns to how people were so effectively manipulated into believing that Arab is a racial category and that Palestinians are exclusively Arab Muslims. That is a spectacular propaganda achievement. It even got me for a while, thanks to the cloistered milieu of the academy.
Rather than calling Gazans “Palestinians,” I have started referring to them as Gazans, a population of Arab Muslims in a territory south of Israel governed by Hamas, a genocidal political movement serving as a proxy of the Islamic Republic of Iran. When you accurately describe the situation, it changes the moral calculus. That is why it’s important to know history and use terms correctly. Ideologues contaminate language to manufacture false perception. A great many people require deprogramming.
Those who mean us harm do the same thing with language around gender. They were effective in changing the meaning of “misgendering” to its diametric opposite. Deceivers are often quite clever. Control over the sense-making institutions is vital not only for manipulating the public, but for unwinding deception. The sane and rational must seize the institutions and reverse the harm the postmodernists have caused.
Today, I watched Anthony Fauci’s testimony before the Senate Homeland Security Committee hearing. He was questioned about his actions during the COVID-19 Pandemic. Fauci asserted his Fifth Amendment privilege. However, a full and unconditional federal pardon, which Fauci received from the Biden regime, removes the witness’s ability to invoke the Fifth Amendment as to the pardoned federal offenses. The man should be placed in irons and hauled before a judge for contempt. But more than punishing contempt is in order. I will come to that momentarily.
For the record, as a professional criminologist, I have spent a great deal of time studying psychopaths. An (honest) expert pegs Fauci as a psychopath within a few minutes of listening to him talk. I trust that even the honest non-expert can see the man for what he is. He is a dangerous man. He lied to the President of the United States and the American public.
Republicans are doing a fine job exposing Fauci’s crimes. Democrats expose their dark ambitions by defending him. I will return to the Senate hearing and what it tells us about the two-party system. But first, I want to say something about the COVID-19 Pandemic and what that period represents. The medical industry killed scores of Americans by intubating them, denying them effective treatments, and jabbing them with experimental mRNA gene therapies with known adverse health effects. Americans watched loved ones die behind thick glass windows because health officials would not let them hold hands with the afflicted as they passed into shadow. Democrats wish Americans would forget all that. We can’t.
The industry denied effective treatments to COVID-19-infected individuals to secure emergency use authorization of mRNA therapies. The administrative state—especially the public health apparatus—allied with the medical industry to conduct an experiment on the population under duress. The major linear and social media platforms, and the progressive-controlled culture industry, served as propaganda organs for the project, suppressing information vital to the public interest and manipulating the masses.
Doctors on trial at Nuremberg
The Nuremberg Code is a foundational ten-point set of research ethics emphasizing voluntary consent, risk-benefit analysis, and the protection of human subjects in medical experimentation. The Code was formulated in August 1947 by American judges during the Doctors’ Trial in Nuremberg, Germany, prosecuting Nazi physicians for atrocities committed during World War II.
Out of the twenty-three defendants prosecuted by the US military tribunal, sixteen were found guilty. Of those convicted, seven were executed by hanging on June 2, 1948, at Landsberg Prison in Bavaria. Five of those executed were licensed physicians. Two others were high-ranking Nazi administrators. Most who perpetrated medical atrocities were spared. Holding them responsible would have required an enormous operation.
Anthony Fauci appears before the Senate
What occurred during the COVID-19 Pandemic, at the direction of Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases (NIAID), Chief Medical Advisor to the President, and Chief of the NIAID Laboratory of Immunoregulation, was a textbook violation of the Nuremberg Code. By issuing Fauci a full and unconditional pardon, the Biden regime admitted to knowing what the man had done. That makes Biden and the regime complicit in his crimes.
But the regime is complicit in more crimes than that. The fascist moment America experienced during this episode involved much more than lying to the public about COVID-19—its origins and the response. Among other elements of fascism were lockdowns, compulsory masking, forced social distancing, mandatory medical procedures, and the delicensing of dissenting health care practitioners.
I wrote extensively about this on Freedom and Reason during the pandemic. WordPress allows its users to publish dissenting opinions. But WordPress is exceptional in that regard. Elsewhere, ideological conformity was required. Those who dissented were punished. People lost their jobs, licenses, and reputations. More broadly, the population was enlisted in the campaign to silence dissenters, publicly ostracizing and shaming them. Families were pitted against themselves.
Dictator: The Hitler Interviews is a documentary series broadcast on Channel 4 that explores the rise and psychology of Adolf Hitler. I watched all four parts last night. I was struck by the parallels to today’s Democratic Party. I will publish an essay about that tomorrow, because other thoughts occurred to me. However, there is a lesson to be learned from a close study of Hitler and the rise of National Socialism: that humanity cannot let this matter go because fascism is not one-and-done.
In the summer of 2020 and for months afterwards, I told readers on my platform Freedom and Reason that America was experiencing a fascist moment. The lesson of the COVID-19 Pandemic makes this obvious: the specter of fascism is a perennial problem.
The specter has been inverted in the minds of millions because of progressive command over our sense-making institutions. But not everybody has been brainwashed. Those watching the Senate inquiry into Fauci’s actions with open ears and eyes can plainly see that the Republican Party is the party of anti-fascism. On the other hand, one after the other, by deflecting and pivoting, Democrats were seen endorsing fascism. If Democrats regain power in 2027, they will return the American Republic to the fascist path. Democrats are the enemy of a free people. This must be said. America must be warned.
When the left portrays Donald Trump as a Nazi, it is projecting upon its enemies its own desire. The spirit of the Democratic Party finds its historical analogy in the totalitarian ambitions of National Socialism. It must conceal this ambition by accusing the Republican Party of it. Affinity with fascism also explains why the Democratic Party embraces Islam, as well as the rising antisemitism in its ranks. During WWII, Islamists aligned with Hitler’s ambition. And Jews were the common scapegoat.
The lessons of history only matter when a people acknowledge them. Those of us who heed the warning must hammer home the lessons. Those who deny or revise history must be ridiculed and shamed.
George Orwell
“If you want a picture of the future, imagine a boot stamping on a human face—for ever.” This quote from George Orwell’s Nineteen Eighty-Four, spoken by O’Brien to Winston in the Ministry of Love, encapsulates the Party’s vision of a future founded on absolute power and control. The Party in Orwell’s novel was Ingsoc. Ingsoc carries a different name today: the Democratic Party.
Orwell’s novel is a work of fiction. But it declares a definite truth. Orwell’s book moves so many people—at least those who care about dignity and freedom—because it speaks this truth. However, too many people see that truth only in Orwell’s fiction and selected historical cases. They do not admit it where it matters most: in the present circumstances. They work not from principle and truth but from partisanship and ideology. They seek power. And what they will do with that power will be terrible.
The nightmare of the Soviet Union began with the Bolshevik Revolution. There are many on the left today who wish something like that would happen again. But a revolution is not necessary. Hitler and his party did not acquire power in Germany in the same way. They were elected to office. The Nazis became the largest party in the Reichstag in July 1932. Once that had occurred, the Nazis established a dictatorship.
There were many opportunities along the way to stop Hitler’s ambitions. But it could have all been avoided if Germans had rejected Nazi Party candidates at the polls. But the Germans weren’t thinking clearly. Their minds had been disordered by ideology and resentment.
The lesson of Nazi Germany is that it is incumbent on each of us to defend our free republic. But to do that, a man must first get his head on straight. He must endeavor to know the time. Grasping the truth of history is a vital part of this. One need not turn to the twentieth century for this history (albeit that period is instructive, which is why I have recounted it here). One must only remember what happened a half-decade ago. Understandably, many citizens want to put the COVID-19 Pandemic behind them. But they can’t. It was a harbinger of things to come.
And, for God’s sake, pass the SAVE America Act. Even if the straight-headed people vote, their vote may not count if our elections are not secure. That’s another thing Democrats would like to leave to the shadows of history: the 2020 presidential election.
* * *
In January of 2025, Newsweek asked, “Why was Dr. Fauci’s Pardon backdated to 2014?” Here’s why:
In October 2014, under Barack Obama, the White House Office of Science and Technology Policy and the Department of Health and Human Services (HHS) halted new federal funding for gain-of-function experiments that could make SARS viruses more transmissible or lethal in mammals. That same year, EcoHealth Alliance began funding and routing bat coronavirus research work to the Wuhan Institute of Virology in China under an NIH grant titled “Understanding the Risk of Bat Coronavirus Emergence.”
The pardon was designed to grant immunity to Anthony Fauci for any involvement in the weaponization of the SARS family of viruses. An investigation into Fauci’s activities would have brought to popular attention US-China collaboration in the weaponization of viruses. This is why Fauci asserted the Fifth Amendment. It was not because he risked self-incrimination. What was at stake was the truth about what the US government had been doing all those years.
* * *
X Preview:
This Fauci thing is massive. Now we know why President Joe Biden issued a preemptive, full, and unconditional pardon to Fauci on January 20, 2025. The pardon covered any federal offenses related to Fauci's medical and public service from January 1, 2014, through January 20, 2025.…
The argument that we must recognize trans-identities because of suicidality—“Do you want a daughter or a dead son?”—is wrong for (at least) three reasons: emotional blackmail, demanding people lie, and misleading the public on the true cause of the high rates of suicide in this population. Emotional blackmail promotes suicidality by valorizing it as a weapon disordered personalities may use to manipulate others to get what they want. We see the same thing with threats of violence against those who refuse to lie about gender. Indeed, suicidality is a threat of self-violence blamed on those who conform to the truth of gender. The reality is that the disordered personality is the true source of suicidality.
Before I get to these three reasons, for perspective, I want to say something about suicidality in minority populations generally. The trans activist argument is that suicidality is high in trans-identifying individuals because of social stigma and rejection. Yet suicide rates for black Americans were lower than for white Americans during the period of Jim Crow. Moreover, while suicide, suicidality, and acts of self-destruction did occur among enslaved people before Emancipation, it was not as common as one might assume given the brutality of slavery. This is an important finding in sociology: populations can endure extraordinarily severe oppression without exhibiting exihibiting elevated rates of suicidality or suicide.
Would the queer community argue that gender nonconforming people are historically more oppressed than black Americans under Jim Crow or chattel slavery? How would they explain the fact that, since the late 1990s and especially after around 2010, suicide rates have increased among black Americans, where before they were lower than for whites, with the sharpest increases occurring among children, adolescents, and young adults? What explains this paradox?
The queer community will blame high suicidality among trans-identifying individuals on alienation from community and family. But suicidality among blacks and mental illness, substance abuse, etc., were lower in the past because individuals conformed to societal expectations. Such conformity was necessary for acceptance by community and family. Community integration, family structure, religious participation, and, crucially, cultural attitudes toward suicide provided the stable environment associated with good mental health outcomes. This last factor is vital. The black community did not promote suicide as an act of resistance or a subcultural alternative to prevailing norms but instead condemned suicide.
* * *
Imagine a white man who demands that others regard him as a black man. Plainly, he is white, so most people would decline to honor his wishes. Suppose he says that if people do not regard him as a black man, then he will kill himself. Should that make a difference? Hardly. A healthy society does not allow people to blackmail others into doing something the community doesn’t believe in. A healthy society expects that the white man must come to terms with the race he was born into. A healthy society does not pretend with the man that he is something he is not and can never be.
Second, it is wrong to demand that people lie or face punishment for telling the truth. It is possible that those who honor the request of a man to regard him as a woman are not lying because they really believe he is (hard to believe, but people are capable of believing the most absurd things). But others know it is impossible, and therefore the demand is that they lie. It is unethical to compel people to lie. It is generally wrong to even ask them to. It is never okay to tell people that they cannot speak the truth. This is the difference between a free society and an authoritarian one.
Third, the appeal to self-harm misattributes the source of suicidality in this population. Research has consistently found that those asserting trans identities have one or more psychiatric comorbidities, including bipolar disorder, major depressive disorder, schizophrenia, and personality disorders—what psychiatry classifies as Cluster B types: antisocial, borderline, histrionic, and narcissistic personality disorders. These illnesses/disorders are all strongly associated with significantly higher suicide rates compared to the general population. more likely to threaten or attempt suicide. The higher suicidality among trans-identifying individuals is not from social stigma surrounding trans identities or resistance to transitioning. It is, moreover, exacerbated by a culture promoting blackmail. When society did not valorize the threat of suicide for this purpose, suicide rates among gender nonconforming individuals were lower.
* * *
There are three things at work here. First, trans is a social contagion in which people are taught to use the threat of self-harm as emotional blackmail. Doctors use the threat to encourage transitioning, from which they profit handsomely. Second, trans activists and the medical industry have moved the locus of suicidality from the illnesses and disorders identified as “gender identity,” an invention of sexology, a project to normalize paraphilias. Third, we know social stigma is not at issue, not only because of the high suicide rates associated with the psychiatric comorbidities (which have grown worse because they are not being treated properly), but also because suicidality is not reduced by transitioning.
This population, whether they transition or not, remains suicidal. That’s explained by the psychiatric conditions associated with transgenderism, not because of trans identification. Telling a mentally ill person to threaten suicide if they don’t get what they want predictably leads to more threats and attempts to harm themselves. The emotional blackmail piece thus makes the problem worse. Moreover, the transition itself plays a role. Realizing that one had made the biggest mistake of his life is expected to increase the likelihood of suicide. Changing his body solved nothing. The suffering of many of those with drastically altered physiology and mutilated genitals is unbearable. Everybody around them betrayed them. They needed help but were instead mutilated and made permanent medical patients. As sociologists have noted for decades, suicide is for many preferable to horror.
* * *
The solution to the problem of trans identification is threefold. First, the medical and psychological industries must stop affirming the delusions of the mentally ill and excusing the behavior or disordered personalities and instead treat the psychiatric condition. In the case of anorexia and cutting behavior, doctors treat the illness. They do not perform bariatric surgery on the anorexic or encourage cutting. The anorexic is not fat. She suffers from a mental disorder. It would be unethical to treat her case any other way, and a physician who affirmed her subjective experience of her condition would face disciplinary action. It follows that doctors and psychologists should be punished with loss of license and prison time for practicing gender affirming care, which is, in truth, gender denying.
Second, we must stop cultural and educational tolerance of trans identification. The government should defund any organization or institution that promotes queer ideology. If promotion of queer ideology persists in public institutions, then the government should shutter them. The state should punish those who groom children to accept perversion. Such persons have no place in a rational and good society. Third, society should not reduce stigma surrounding trans identification (or furry identification, etc.). On the contrary, it should increase stigmatization of paraphilias. Making paraphilias embarrassing and shameful deters others from adopting them.
The big complaint on the far right today—the rogue America First crowd—is that Trump has morphed into a neoconservative. In 2004, I penned two chapters in Bernd Hamm’s Devastating Society: The Neo-Conservative Assault on Democracy and Justice. One of those chapters (you can read the article version War Hawks and the Ugly American: The Origins of Bush’s Middle East Policy on this platform) was a deep dive into neoconservatism and the Project for a New American Century (PNAC) and their plans to instigate a “democratic tsunami” across the MENA space. I know a bit about this ideology.
Trump is no ideologue. He’s a pragmatist. It’s an error to group him with the PNAC crowd of warmongers whose grand vision is rooted in American imperialism and globalism. When Trump said “no new wars,” he was explicitly separating himself from the war hawks; he was not saying that America would never go to war (see Trump Never Promised to Eschew Military Power to Confront Tyranny). Such a stance is suicidal. It allows evil to gather strength. The America Firster who thinks like this is the same America Firster who delayed America’s entry into World War II. Isolation bolsters our enemies’ ambitions. Millions died needlessly because America sat on its hands while Nazi Germany gathered strength. It took the attack on Pearl Harbor to finally move the United States to action.
America bombs government buildings in Baghdad on March 21, 2003 (source image)
The term “neoconservative” is used in popular speech as a synonym for “hawkish” policy or looking favorably upon military action, but historically it referred to a much broader strategic doctrine. The neoconservatives associated with the George W. Bush administration—figures such as Paul Wolfowitz, Richard Perle, Douglas Feith, and others—influenced a vision that extended well beyond removing specific threats.
Crucially, neoconservativism was a rebranding of Cold War progressivism. The ideology was hatched and raised by the Democratic Party and then migrated to the Republican Party when conservatism fully returned from the wilderness following the Great Depression. Neoconservatism corrupted the party. The Bush family was their political vehicle. It then returned to the Democratic Party with Barack Obama’s election. Hillary Clinton was meant to carry the torch for transnationalism. However, there are Republicans in power who remain committed to neoconservative ambition. They loathe Donald Trump.
Even before 9/11, the neoconservatives argued that authoritarianism in the Middle East bred terrorism and that the United States should actively reshape the region by overthrowing hostile regimes and fostering democratic governments. This is not altogether untrue. The question is how America and the West should address the problem. For neoconservatives, the invasion of Iraq was presented not merely as eliminating Saddam Hussein or addressing alleged weapons of mass destruction (which Hussein did not possess), but as the first step in a “democratic domino effect” that would transform Iraq into a model for political liberalization throughout the Middle East. This ambitious project was often described as the “Freedom Agenda.”
Trump’s approach, by contrast, has generally not been framed in those transformational terms. Although he authorized significant military actions—including the 2020 strike that killed Qasem Soleimani and later strikes against Iranian-linked targets—his rhetoric has consistently emphasized deterrence, retaliation, and protecting American interests rather than remaking the political order of the Middle East. Even when using force, Trump has repeatedly stated that he does not seek long-term nation-building or regime-change occupations. His foreign policy has tended to combine military assertiveness with skepticism toward prolonged interventions, reflecting a transactional worldview rather than the ideological internationalism that characterized neoconservatism.
This does not mean there is no overlap, as alluded to above. Islam is an existential threat to the world. Both Trump and the neoconservatives have at times endorsed the use of overwhelming military power, maintained close strategic ties with Israel, and viewed Iran as a principal regional adversary. These are views to which any rational actor may—must—subscribe. Those similarities explain why some observers perceive continuity. However, the underlying strategic logic differs considerably. For the Bush-era neoconservatives, military force was often a means of transforming political systems and spreading liberal democracy, i.e., corporate transnationalism. For Trump, military force has generally been presented as a tool to punish adversaries, deter attacks, or eliminate perceived threats without assuming responsibility for rebuilding societies or exporting democratic institutions.
Describing Trump as a neoconservative solely because he ordered military action against Iran conflates tactical decisions with grand strategy. The defining characteristic of neoconservatism is not simply a willingness to use force but a belief that American military power could and should be used to reshape international politics by promoting a simulation of democratic governance. Unless one sees Trump’s actions as part of a broader commitment to regional political transformation, the comparison is faulty. The evidence that Trump is committed to regional political transformation just isn’t there. A more precise characterization is that Trump has at times adopted policies resembling neoconservative tactics while rejecting the larger ideological project that made neoconservatism distinctive.
America bombs Tehran, Saturday, Feb. 28, 2026. (Image source)
As for neoconservatism, it will not escape the reader who reads my chapter in Hamm’s book that, at the time I penned those words, I was not a supporter of intervention in the MENA space. I have softened my view on military intervention after consideration of the threat Islam poses to the world. More than twenty years have passed between then and now, and the advance of a barbaric ideology has made considerable strides in capturing the West. This does not make me a neoconservative, but rather it aligns me with, as I put it in the April 2026 essay, Donald Trump’s Grand Vision: Make Western Civilization Great Again. It’s not as if Trump didn’t explain it to his MAGA followers. Where was panic then? Did they not read Trump’s National Security Strategy and the Case for Democratic Nationalism? In truth, Trump’s vision is America First without the isolationism that corrupted the first iteration. Trump is a pragmatic nationalist.
There is nothing in Trump’s actions on Iran that contradicts his long-held position on war. Indeed, it is very clear that he did not want to have to deal with Iran and that he is trying to find a way to bring the Islamic Republic to the table and negotiate a resolution to the problem of Iranian belligerence and the desire to acquire nuclear weapons. However, the events of October 7, 2023, in which Hamas, an Iranian proxy, invaded Israel and massacred civilians in the most horrific ways imaginable, changed the situation. Iran is the chief sponsor of international terrorism. Its goal is the destruction of Israel and the West. (See Israel and the Existential Threat of a Determined Iran.)
There is nothing intrinsically wrong about regime change when that regime seeks world conquest and nuclear weapons (see US Strikes Iran’s Nuclear Facilities). The West, with America leading the charge, changed regimes in Germany and Japan during World War II. Regime change in Iran is a perfectly reasonable objective. At the very least, the Islamic Republic needs to be defanged and put on a tight leash. If we want a safer world, the West must confront Iran and Shi’a Islam—not just abroad, but at home. Europe should join the fight (see Not a Modest Proposal: Repurposing NATO for the War on Islamofascism).