

I have seen this meme now several times. Pay attention to language. SARS-CoV-2 is a virus, not a bacteria. Bacteria are much bigger than viruses (by at least a factor of ten). Viruses range in size from 0.02 to 0.25 micron diameter. Bacteria are also much less likely to be aerosolized than viruses. They are heavier and fall downward at a faster rate. This is why surgeons use face mask, so that bacteria do not fall from their noses and mouths and contaminate surfaces (or are less likely to do so). Aerosolized viruses are not in the form of respiratory droplets that masks are designed to stop. That’s why that other meme showing the man pissing on another man’s leg is so absurd. Aerosolized particles are nothing like urine. Viruses easily go through and around the sides of masks. Wearing a mask to stop a virus is like trying to keep out mosquitos with a chainlink fence.
Because viruses are so small, they remain in the air for days. Inside. Not outside, where sunlight kills them. Inside, where the experts told everybody to go. Viruses accumulate inside. So when you’re at the grocery store with your mask on, and there have been people in the store with COVID-19, you are walking through aerosolized virus, suspended for an even longer time thanks to constant airflow. Your mask does not protect you.
Watching lectures by industrial hygienists on the efficacy of masks vis-a-vis viruses (for example, see above), it becomes obvious that the obsession with masks amounts to a ritual act in the worship of the corporate state. Masks are like hijabs. Both function to avoid offending powerful entities that limit freedom for the sake of glorifying control. The only things wearing them will protect you from are shame and discipline.
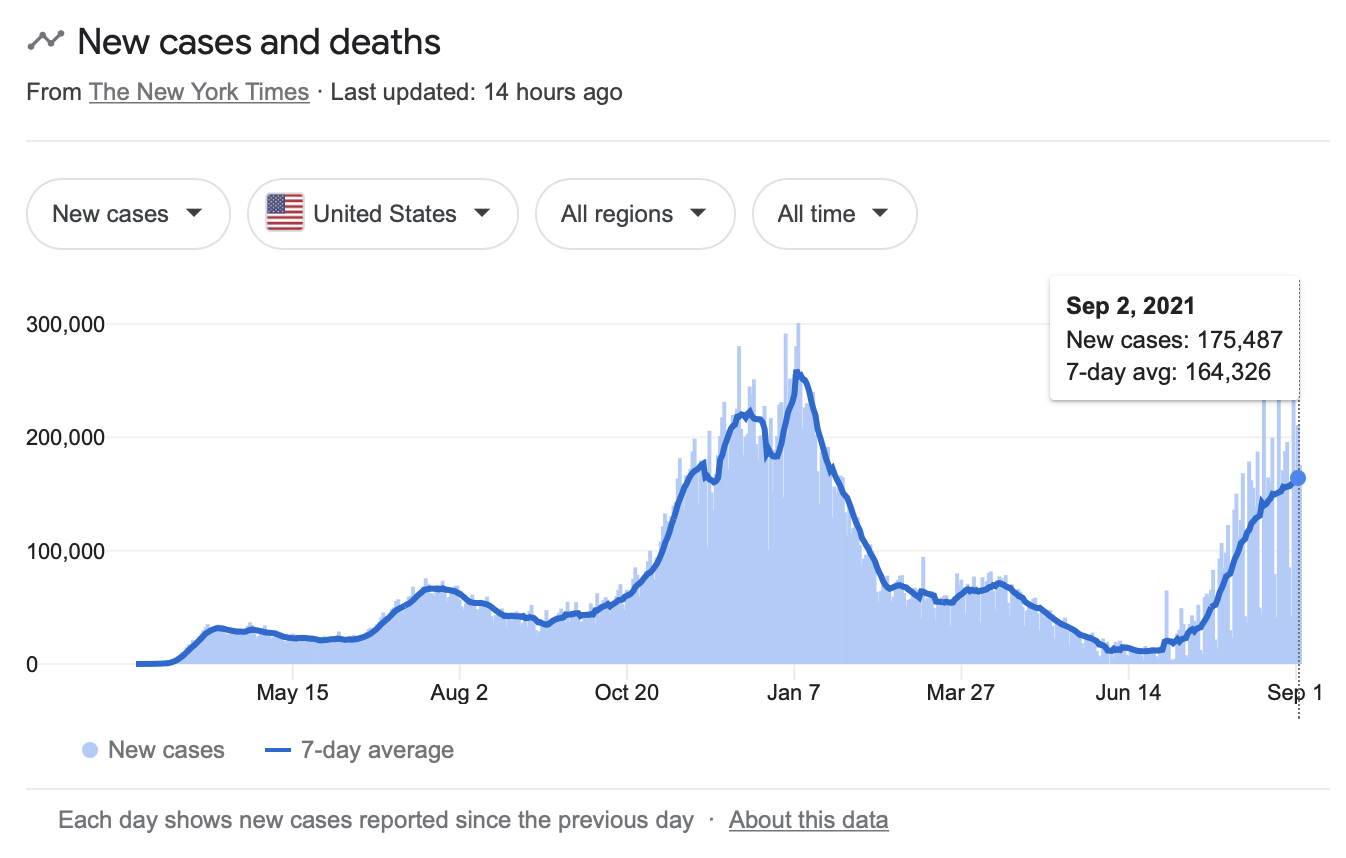
There are some other useful conclusions to draw from what industrial hygienists are teaching us. First, most people have been exposed to this virus repeatedly but not everybody who is exposed gets sick. Why? It is likely that, since most of us have had coronavirus infections throughout our lives, we already enjoy some immunity from it. As I have explained on Freedom and Reason, coronaviruses are among the several viruses that causes the common cold (rhinoviruses and adenoviruses are other common cold pathogens). This means the R0 associated with SARS-CoV-2 is low compared to, say, the R0 with measles. I am not choosing the most extreme R0 to make the comparison. Anthony Fauci is the man who argues that SARS-CoV-2 is so contagious that we need to reach the same vaccine coverage as measles (around 95 percent) to reach herd immunity. SARS-CoV-2 is more in the R0 range of the flu. That means that, if these vaccines work, a big if, we surpassed herd immunity by virtue of the numbers vaccinated so far, approaching 55 percent for fully vaccination, with more than 60 percent having received at least one shot, which expects tell us has a significant degree of efficacy. But the vaccines are leaky, which means that they don’t prevent infection. The likely reason why we are back where we were during the peak (see chart below) is leaky vaccines that keep the vaccinated healthy enough to get out in the world and spread the virus and, moreover, keep the more sickening strains from being victims of natural selection.
* * *
According to the CDC, during the 2018–2019 season, 136 deaths in children with laboratory–confirmed influenza virus infection were reported in the United States. The CDC notes that influenza-associated pediatric deaths are likely under-reported as not all children whose death was related to an influenza virus infection may have been tested for influenza. Using several sources of data, the CDC estimates that there were approximately 480 deaths associated with influenza in children during 2018–2019. For the 2017-2018 flu season, 186 pediatric deaths were reported, which was the highest number since the 2009-2010 season, where 348 pediatric deaths were reported. The CDC does not estimate numbers for these other seasons in the report, but if they look anything like the estimates for the 2018-2019 season, then the numbers of pediatric deaths in any of them greatly exceed pediatric deaths from COVID-19.
COVID-19 involves vastly higher rates of testing, so the need to estimate is not as pressing. As of August 26, 4.8 million children had tested positive for COVID-19. To date, taking the greatest range of ages that could conceivably be classified as children (0-18), there have been 470 pediatric deaths during the pandemic. Keep in mind that this is over an eighteen-month time span, a much greater timeframe than any flu season (ask yourself why they are doing a continuous run of disease and death with COVID-19 and not breaking it up into seasons like influenza, which is also a continual thing). This means fewer pediatric deaths over a longer period of time from COVID-19 compared to influenza. The pediatric case-fatality rate for children is 0.00979. The infection fatality rate is considerably less than this. And they want to mandate masks and vaccines. We locked down schools for this.
* * *
According to the CDC, the average number of serious health conditions, or comorbidities, associated with COVID-19 deaths is four? as I have reported before, according to the CDC, only five percent of those who have COVID-19 listed on their death certificate died of COVID exclusively. This is why it is important to eat right and exercise. Obesity is a real killer. But should we mandate it?
I got push back for this. A pregnancy is not contagious. This, of course, misses the point. The principle in question is bodily autonomy (libertarian concern) over against harm to others (communitarian concern), not whether pregnancy is contagious. If one is going to argue that the state can violate a person’s bodily autonomy for the sake of other people on a medical matter, then the argument about abortion is lost. The fetus is alive. It is a human by virtue of its genetics. Abortion kills a human. Therefore, the woman’s body can be controlled for the sake of the fetus.
That’s the wrong argument. Totalitarianism flows from the abandonment of the principle of bodily autonomy. It makes people pawns of technocratic goals, of public health authorities (who, quite clearly, are not oracles). This isn’t at all like a man who intentionally harms others. Imagine the state commandeering our bodies to support the lives of those with diseased kidneys. It’s not my fault somebody’s kidneys are diseased. They can’t have one of mine. Indeed, the case against abortion is much stronger than the case for vaccines because vaccines are imposed on healthy people who may not get infected (and may be injured by the vaccine), whereas an abortion is almost guaranteed to kill a human being (there have been a tiny percentage of fetuses that survived an attempted abortion). And hundreds die every year waiting for a kidney, while most people have two functioning ones. Isn’t society killing people with kidney disease by failing to use other people’s kidneys to save them?
COVID-19 is not the only contagion. There are a myriad of pathogens transmissible through human contact. If that’s the principle, then we should mandate vaccines for each and every vaccine produced by Big Pharma—and administer all available antivirals for those who testing positive. HPV for men. Who cares if they don’t have a uterus. His body must be clean for others. Etcetera. It won’t do to say that COVID-19 is more serious than all those other pathogens—as a factual matter, it’s not. In fact, if you are not obese, then you will are almost certain to survive COVID-19. So why don’t we regulate civilian food intake? Why don’t we poke people with sticks until they get off the couch? No, we instead recommend people diet and exercise and get a vaccine. If they don’t to do these things, that’s on them.
Even if one wanted the argument to be about contagion, it is clear at this point that there is COVID-19 vaccine in existence or in the conceivable future that prevents infection and transmission—or even sickness and death—from SARS-CoV-2. It’s like influenza, rhinoviruses, adenoviruses, etc. (all potentially lethal, by the way). Look at the trend lines in the above chart. The vaccine not only isn’t working, but it’s increased use is associated with a rise in cases. Are the causally related? Could be. There’s a compelling argument about that. However, we are now back where we were when COVID-19 was at its worst, and it’s not because people aren’t getting vaccinated.
The communitarian argument crashes not only on the rocks of bodily autonomy, but upon the spiked protein of a leaky vaccine. What the vaccine does do is make people who are infected less sick. If a person wanted to reduce his personal risk of getting sick, he’d think about the vaccine and weight the risks. Same with going on a diet and exercising. But that’s up to the individual.
It has pointed out to me as if I didn’t know that the Supreme Court has long held that the state has the power to compel vaccination. See my essay The principle that sustains compulsory vaccination is broad enough to cover cutting the fallopian tubes, where I analyze the Supreme Court decision, Jacobson v. Massachusetts, 197 US 11 (1905), the decision that upheld state government’s power to compel smallpox vaccination, ruling that, under certain circumstances, citizens are subject to the police power of the state on matters of public health. Despite the very narrow constraints the decision placed on state power, the Supreme Court has since interpreted state power to compel vaccination—and other things, including forced sterilization—broadly.
As I wrote in that essay, “Every third person died from smallpox, and the rate was even greater for babies. Survivors were often blind and scarred for life. The modern smallpox vaccine, developed in the nineteenth century, is a live virus preparation of the vaccinia virus, which is safe and cross-protective for cowpox, monkeypox, and smallpox (variola). The smallpox vaccine is effective in preventing infection in 95 percent of those vaccinated. Get back to me when SARS-CoV-2 becomes that lethal and there is a vaccine that successful.”
(See The Official Vaccine Narrative Completely Falls Apart; The Immorality of Vaccine Passports and the Demands of Nuremberg; The Communitarian Nightmare We Feared is Here; Somehow, a Bill of Rights got Locked into the Constitution.)

My quick-and-dirty mask heuristic: even if they are theoretically able to slow the transmission of an airborne virus no one seems to take into account or care about real-world mask wearing: ill-fitting, and infrequently changed.