A short while ago, the jury in the Ahmaud Arbery death case, a murder that occurred on February 23, 2020 in Satilla Shores, a neighborhood near Brunswick in Glynn County, Georgia, reached its verdict. Travis McMichael, who shot fatally shot Arbery, was convicted on all nine charges, including malice murder and four counts of felony murder. McMichael’s father, Gregory McMichael, was found not guilty of malice murder, but was convicted on the remaining charges, including the felony murder counts. The McMichael’s neighbor, William Bryan, was found guilty of two of the felony murder counts and a charge of criminal intent to commit a felony. The killers were white. Their victim was black. The general view will be that justice was served in this case, although I suspect there are some who believed a different outcome would be more useful for their political purposes.

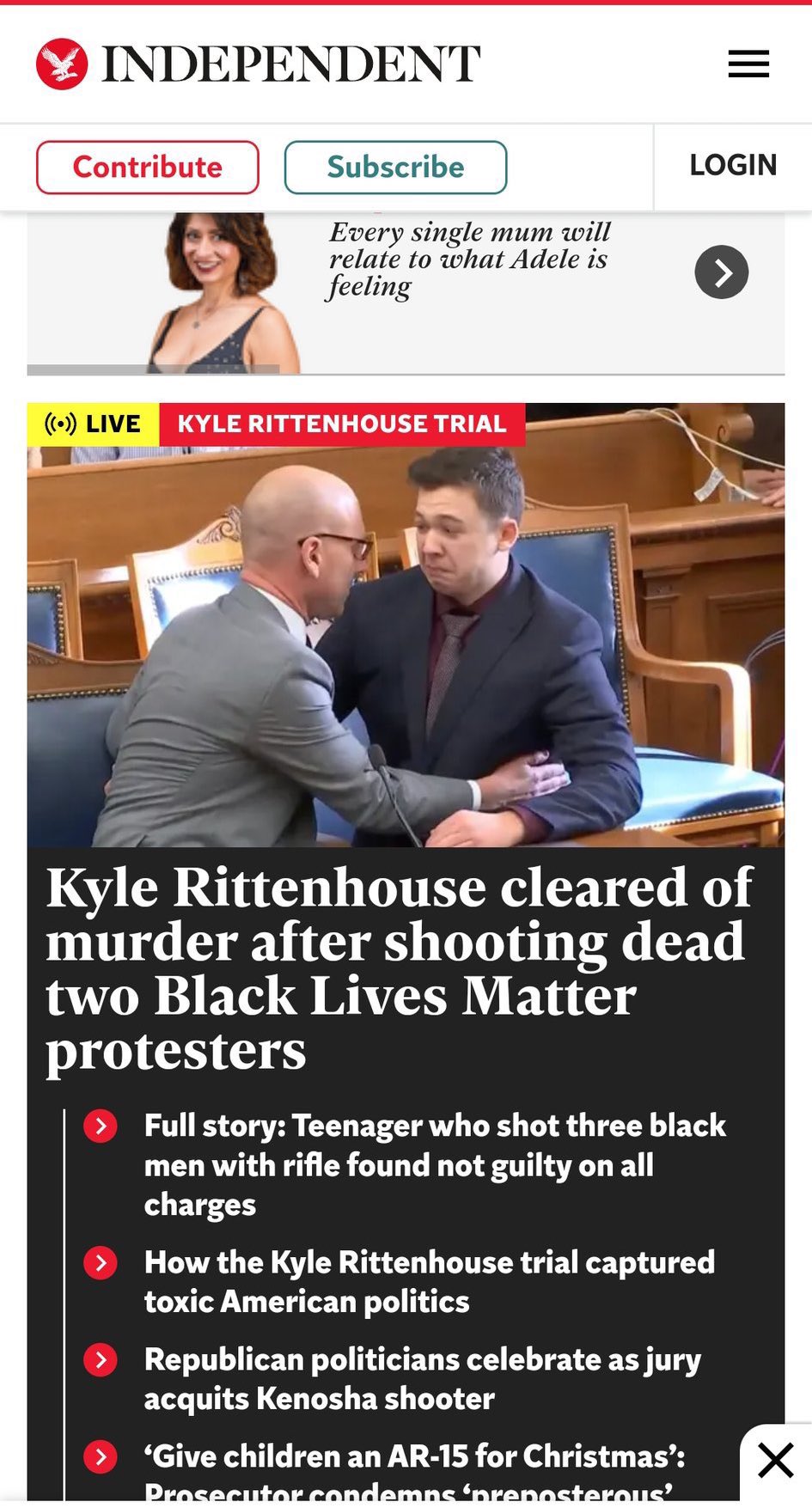
As was the case in the trial of Kyle Rittenhouse, the jury being able to see video evidence makes a hell of a difference. You might have wondered why, then, with facts and reason demanding Kyle Rittenhouse’s acquittal on all charges, the establishment still refuses to acknowledge that justice was obtained in this case.
Context matters. Kyle Rittenhouse’s crime was standing up to the mob that the corporate state and the progressive rank-and-file had enabled. The criminals who assaulted him that night were doing the bidding of the establishment. Their task was disordering the community of Kenosha, as they had disordered so many other communities in the weeks following George Floyd’s murder under the weight of Minneapolis police officer Derek Chauvin in May of 2020. The establishment can’t try Rittenhouse for interfering with a color revolution. They can only defame him for doing a noble thing. And so they did. And so they continue to.
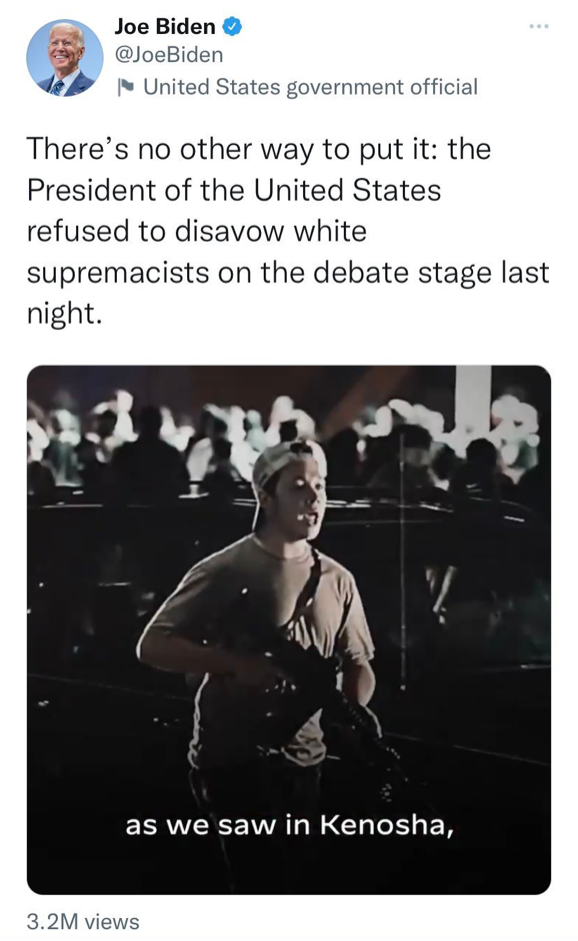
This is how corporate state propagandists portrayed Rittenhouse upon his arrest:

How ideologically deranged does one has to be to find something untoward about Blue Lives Matter imagery and possessing Armalite rifles? As if supporting the police and the Second Amendment are indicative of a terrorist mentality instead of a young patriotic man who embraces the ethics of public safety and self-defense. Of course, patriotism, public safety, and self-defense are the problems. Patriotism is anathema to transnationalist desire. Public order is the antithesis of the disorganized community those who thrive on chaos seek. The right to self-defense presumes the ethic of individual autonomy, a moral barrier to serfdom.
Rittenhouse was guilty from day one and no fact was going to change that narrative. And so it didn’t. In a November 19 publication, the American Civil Liberties Union complained that “Rittenhouse was not held accountable,” presuming a guilty verdict was appropriate in that case. The author of the essays, Leah Watson, a staff attorney, writes that “Kyle Rittenhouse didn’t act alone.” Who else was in on it? The mob that was burning, looting, and vandalizing the city? No, law enforcement was Rittenhouse’s accomplice. Watson claims that the actions and inaction of the Kenosha Police Department and the Kenosha Sheriff’s Department played a critical role in the tragic events that took place. Indeed, it was the inaction of law enforcement and emergency services that caused Kyle Rittenhouse and other young men to step up to the task of putting out fires and administering first aid. But Watson didn’t mean that.
Misrepresenting the shooting of Jacob Blake, Watson writes, “Faced with this latest manifestation of law enforcement’s systemic mistreatment and disregard for the lives of Black and Brown people, people took to the streets of Kenosha.” On August 23, 2020, police were dispatched to the scene of a domestic disturbance (the 911 call indicated a very serious situation) whereupon they discovered the man they were detaining had a warrant for criminal trespass and sexual assault with domestic abuse as modifiers. Attempting to affect an arrest, which became physical and saw the deployment of a Taser, Blake, armed with a knife, wrestled free and was moving with purpose to a vehicle that may or may not have been his. There were kids in that car. Black was either reaching for a gun in his car or trying to leave the scene with those children when he was shot. Blake survived his gunshot wounds (the media routinely report the shooting as a killing). The police did the right thing. But that’s not how the media reported it.
“Make no mistake,” Watson opines, without the benefit of supporting evidence, “the shooting of Jacob Blake and the related protests and fatalities stem from the deep-seated white supremacy that pervades our criminal legal system.” Aware that there is no evidence supporting the claim, Watson appeals to a false historical narrative “that recalls the origin of American police in slave patrols” (see The Line from Slave Patrols to Modern Policing and Other Myths). “These patrols sought to capture and return formerly enslaved people to the violence of enslavement and their later connections to white supremacist agitation during the Civil Rights movement are echoed in the violence seen in Kenosha.” Whether true or not, what does this have to do with Kenosha? According to the ACLU, contrary to what it known about the night, “white people brandishing weapons of war are given the benefit of the doubt and even encouraged by officers of those same police agencies.” This is what The Daily Beast sees in Blue Lives Matter imagery and Armalite rifles. They need only to see a young white man who believes in the rule of law to fill in the rest. This is the logic of identity politics. It’s not what you do. It’s who you are.
Watson applies a normative claim to a misrepresented situation: “Law enforcement should play no role in protests, unless it is to protect our First Amendment rights, and they should not use violence to control the crowd or silence those they disagree with.” Arson, destruction of property, looting, vandalism, and assault are not First Amendment expressions. They are criminal acts. Law enforcement has a duty to act under those circumstances. Members of the mob were armed, as well—and they were the aggressors. They came to Kenosha to commits acts of destruction and violence. It’s what Antifa and Black Lives Matter do. Rittenhouse and those like him were in Kenosha that night because inaction by public authorities green-lit violent political action. Rittenhouse was attacked because he was preventing little fires from becoming big fires and removing hateful slogans from buildings. The ACLU exists in a space safe from reality.
As you can see in the video below, Joseph Rosenbaum, the first man to attack Rittenhouse, became enraged when a member of the group Rittenhouse was with, armed with a fire extinguisher, put out a fire in a dumpster that Rosenbaum had lit. Rosenbaum and the mob was pushing the burning dumpster towards police cars down the street. “Why did you do that?” Rosenbaum demanded to know of the individual who thwarted their action. Because the police were standing down and citizens have a duty to defend their community. Watson tells an entirely different story, which you can read here. (For the record, I recently resigned from the board of the Northeastern chapter of the ACLU in protest of the organization’s abandonment of its traditional concern for civil liberties and rights. The ACLU has only gotten worse since then.)
Those who support the mob see Rittenhouse as a bad actor for putting out fires. In a blatant expression of victim blaming, they agree with those who attacked him that he should not have acted to diminish the impact of mob action. Who are these people who seek to maximize the destruction of the mob for political purpose? I have already identified them. They represent the corporate state and the progressive establishment. Academic, cultural, media, and political elites encourage the mob. They declare the mob righteous. Kyle Rittenhouse is the antithesis of the mob, the living personification of their ideological enemy. He is guilty because of who he is and what he represents. Working class white males are oppressors. Oppressors forfeit their rights. (See The Establishment Project to Demonize Conservative White Males. What’s This All About?)
As I argued in yesterday’s blog (Waukesha is Scheduled to be Memory Holed), the power elite are conditioning the masses to assess threats to their safety in ways that serve the interests of the corporate state. Although the character of racism has changed since the nineteenth century, shifting from anti-black to anti-white, this is not true for the character of classism; the working class remains the dangerous class. Mapping the shift in racism on top of classism we now have the problem of the white working class. This has been in the making for quite some time. Long-time readers of my blog will remember my essays on the problem of Islam and the efforts of progressives to downplay the significance of Islamic terrorism while promoting the Islamization of the West. This effort has involved denigrating white Christians, who are routinely portrayed a bigots for expressing concerns about Islam’s treatment of women and children. There is a common political economic interest underpinning the rationalization of the threat of black nationalism and rationalization of the threat of Islamism. Promoting Islam and black nationalism are part of a long-standing project of weaponizing minorities against the white working class Christian majority.
I write this as a life-long atheist, a religious pluralist, and an advocate of racial equality. I have no interest in Christianity being the dominant religious force in the West beyond a concern for what will fill the vacuum left by its marginalization (and that includes not just other recognized religions but such quasi-religions as antiracism). As for whiteness, I desire to live in a world were race doesn’t matter. But anti-white racism has become a hammer in the corporate-state toolbox. As I have said before, I don’t want to talk about race and religion, but others make me. As a man designated white at birth, anti-white racism represents a risk to the health, safety, and well-being of my family. It’s personal. I have to speak up.
Understanding the corporate-state project of anti-white racism helps us explain a lot of things. The promotion of anti-white racism is how the goals of assimilation and integration get redefined as racism and replaced by such divisive practices as diversity and equity. This is how Muslims become a race and the terroristic acts of black nationalists denied and downplayed. This is not a conspiracy. Those who say this mean to confuse the public. The project is open and in our faces. Today, it’s mainstream policy and practice. Organizations require workers to attend struggle sessions, euphemized as workshops and training in diversity, equity, and inclusion, where they are shamed for their whiteness. The assumption we are all supposed to make fundamental to our cognitive and moral processing is that whites are the bearers of white supremacy who enjoy a race privilege at the expense of black people for whom riots are the language of the unheard. Critical race theory explicitly makes this argument. We’re told that systemic racism is a real thing, that it is everywhere, and that white people uphold it in their defense of the Enlightenment, exposed as the racist project of white people. They’re teaching children this. When you object you confirm the truth of the accusation. If you object at a school board meeting, you are a domestic terrorist.
Eric Garner’s son has condemned a Black Lives Matter leader Hawk Newsome for threatening “riots,” “fire” and “bloodshed” if Mayor-elect Eric Adams resurrects the NYPD’s anti-crime efforts—calling it “an insult to my family and the movement at large.” “Hawk Newsome threatening to burn down our city in response to Mayor-Elect Eric Adams’s proposal of bringing back the anti-crime unit in plain clothes is an insult to injury to my family and the movement at large,” Garner said. Garner’s remarks, while I am sure are heartfelt, reflects an attempt to rein in Black Lives Matter for public relations purposes. But it’s the movement itself that is the problem. It is a racist anti-working class movement organized and bankrolled by corporate power. Black Lives Matter’s explicit reasons for existing are based on falsehoods that slander and libel criminal justice professionals and white people.
A moment ago I dropped the word “terrorism.” The meaning of that term may feel slippery to many readers. In criminology, however, definitions enjoy precision. As it happens, I know a lot about this. Terrorism is the subnational use of violence or the threat of violence, especially against civilians, in the pursuit of political ends. A terrorist is a person who resorts to such means and methods to produce a state of fear or submission. Examples of terrorism: (1) a black nationalist driving his car into a Christmas parade and swerving to hit civilians; (2) a black nationalist threatening to burn down New York City if the mayor gets tough on crime; (3) black nationalists threatening jurors with bodily harm if they return a verdict of not guilty in the case of white defendants claiming self-defense in the shooting of a black man.

With (3), I do not mean to imply that the presence of Black Lives Matter and the New Black Panther Party outside the Glynn Country Courthouse produced the desired verdicts. It was the intent of their presence. I also do not mean to imply any new limitations to the First Amendment. True threats are not protected by the First Amendment. A true threat is a symbolic action meant to cause one or more specific persons to believe they will be seriously harmed by those intending to engender that belief. The purpose of a true threat is to frighten or intimidate one or more specified persons into acting in a manner desired by the frightener. This is the point of terrorism (see above).
We are hearing quite a lot about white nationalism these days. In covering for Buzzfeed News the civil trial in Charlottesville where a jury just ordered white nationalists to pay 25 million dollars to victims of the “United the Right” rally, Christopher Miller writes, “The verdict in the landmark trial comes amid a resurgence of far-right domestic violent extremism and the mainstreaming of these ideologies, ushered in by Donald Trump. The former president’s hyperpolarizing populism, nationalism, and racist rhetoric has enabled his followers—and some elected Republicans—to endorse violence, including an attack on the US Capitol in January.” I am tempted to explain why everything Miller writes in his essay is exaggerated, false, and misleading, but I have been over the ground many times before. There’s a more pressing matter today—the clear and present danger of black nationalism.
Black nationalism is at least every bit as dangerous as white nationalism. Indeed, while the white nationalist threat is overblown, black nationalism is in ascendency. It just killed and injured scores of people in Waukesha, Wisconsin only a few days after Rittenhouse was acquitted on murder charges. It wasn’t white nationalism that led the destructive and deadly political violence occurring throughout the summer and fall months of 2020. Political violence through May 26-June 8 alone is estimated to cost at least two billion dollars. Where is the trial ordering black nationalists to pay for that destruction? Worse, more than two dozen people were killed over those months of mob violence, violence that wasn’t condemned by the establishment but celebrated and encouraged. Where are the high profile criminal trials holding the perpetrators responsible? The media is asking former Vice-President Joe Biden whether he wishes to take back his characterization of Kyle Rittenhouse as a “white supremacist.” When will the media ask Biden if he takes back his characterization of months of mob violence as “peaceful protest”? As noted in yesterday’s blog, “If you can’t see the massive double standard, then you’ve poked out your eyes.” Ideology will do that to you.
If I replace black nationalist with white nationalist in the examples I give above, one has has no trouble seeing the terrorism. I have written about white nationalist terrorism. In many cases, hate crime charges are brought instead of terrorist charges. Progressives are horrified by the reluctance of authority to charge violent white nationalists with terrorism. They rightly wonder (in light of their perception), Why dark skinned Muslims but light skinned Christians? But changing the color or the religion of the nationalist or supremacist doesn’t change the definition of terrorism. We have the establishment eager to attach the label of domestic terrorism to parents complaining at school boards about what their kids are being taught while authorities rule out terrorism almost as soon as they capture to the man who drove his car into a Christmas parade and intentionally swerved to maximize the death toll—this contradiction determined by racial politics.
Americans of all races, ethnicities, and religions have for too long tolerated these forms of extremism, as well as the elite attitude that promotes them. For too long Americans have put up with a double standard that has in back of it project to defame those who extol American values. If we do not rise to speak the truth and confront the lies and expose the double standard, then we will lose our country. The West is in peril, and the forces behind its pending demise are transnational in scope and corporate in character. There’s a New Fascism on the horizon and it’s rapidly approaching. The ordinary America is its target.