Those who were present at the news conference where the man (not Gordon Findlay, the global brand director for Novo Nordisk) fainted reported that, since three doctors were tending to the man, it was not imperative that Kennedy, who is not a doctor, immediately do so.
A rational person understands that not everybody responding to a health crisis has to behave in the same way. But in this age, on one side at least, rationality is only embedded in the system, not in minds. In either case, the behavior is irrational.
On planet earth, what Kennedy did, besides making room (my initial interpretation, since he was not the only one to leave the gaze of the camera—moreover obvious in the handlers shooing reporters from the room, which observers do see), was retrieve a chair. If you watch the sequence of events, the man first started falling, and Kennedy thought he just needed to sit. Kennedy also got a wet towel for the man, too, a common thing to do when an individual faints.
So, no, Kennedy wasn’t fleeing the scene. He was responding rationally to the situation. He’s known as a steady man.
Trump watches doctors tend to stricken man
Why people wrongly interpreted Kennedy’s actions, just as they wrongly framed Trump’s response (which was one of concern, if you don’t rely on a single conveniently curated still image), is a cognitive fallacy known as “motivated reasoning,” where one’s perception of a situation is shaped by an ideological or partisan worldview, often without charity, in this case a worldview eager in every instance to attribute to Kennedy and Trump untoward motives. Those afflicted cannot see it any other way. And the corporate state media leaves them to it.
Concerning Trump’s actions that day: “I wanted to speak to the wife to let her know what was happening, but also comfort her,” Dr. Oz reported. “The president saw me in the corner and said, ‘Who are you talking to?’ I said, sort of sheepishly: I was talking to the wife. And he said, ‘Give me that phone.’”
Yesterday, I drafted an essay concerning the passing of Dick Cheney, a warmonger who held numerous positions in government over the last half a century, most recently as Vice President under George W. Bush (2001-2009), the son of former CIA director and appointed minder of President Ronald Reagan, George H. W. Bush. I hope to publish that essay tomorrow, but the election of Zohran Mamdani as Mayor of New York City pushes it back.
Mamdani is the man on the right
I will, however, provide readers with a bit of a preview because it is relevant here: My forthcoming essay will illustrate why one must avoid dwelling on personalities and instead understand world-historical developments and the dynamics driving their ambitions. I critique Thomas Carlyle’s influential “great man” theory of history. Recalling Georg Hegel’s concept of the “world-historical figure,” Carlyle contended that the actions of extraordinary individuals primarily shape the course of history; society advances because of rare figures whose courage, moral force, and vision enable them to influence the destiny of nations and civilizations. For Carlyle, historical change reflects human greatness, with the masses and social structures playing subordinate roles. Making history is, in his words, “the biography of great men.”
Although I emphasize the role of social structures in shaping historical events and the personalities that appear in our history books, there is something to Carlyle’s thesis. Muhammad, born in Mecca around 570 CE, regarded in Islam as the final prophet, received from the Archangel Gabriel God’s message to humanity. His revelations were later compiled into the Qur’an. Muhammad authorized and personally led numerous military expeditions after establishing Islam in Medina, and over the next decade, the Muslim polity expanded through warfare and the submission of other tribes. By the time of his death in 632, most of the Arabian Peninsula had come under his political and military authority. The regime was cruel and unforgiving. The case of Muhammad is certainly illustrative of the force of personality.
The ambitions and cruelties of Islam did not end there. The attempted Islamic conquest of Europe began soon after the rise of Islam, in the seventh century, as Arab forces expanded rapidly across the Mediterranean. Muslim armies entered Europe through two main routes: across the Strait of Gibraltar into Spain and through Anatolia and the Balkans toward Constantinople. Frankish forces halted further northward advance at the Battle of Tours in 732, but Muslims controlled the Iberian Peninsula for centuries, while Islam spread east and south across the planet.
Muslim rule in Spain ended in 1492, when the Catholic monarchs Ferdinand of Aragon and Isabella of Castile captured Granada, the last Muslim stronghold on the Iberian Peninsula. This event concluded nearly eight centuries of Islamic presence that had begun with the Umayyad conquest in the eighth century. The fall of Granada marked the completion of the Reconquista, the long Christian effort to reclaim territory from Muslim rule, and it coincided with Spain’s emergence as a unified Christian kingdom and global power. Without the bravery of the European Christians, the American Republic would not exist.
Muslim expansion into eastern Europe was largely halted by the strength of the Byzantine Empire, which successfully defended Constantinople during two major Arab sieges, preventing a direct route into the Balkans. Difficult terrain, long supply lines, and the rise of powerful regional forces created rather intractable military and political barriers. These factors together limited further advance and kept Islamic rule from extending deeply into eastern and central Europe during the early centuries of Islamic expansion.
However, Muslims could not be content with controlling much of the world east and south of European Christian civilization (for a map of Islam’s present reach, see my recent article Whose Time Has Come?). In the ensuing centuries, Islamic imperialists recalibrated their strategy of attack, in recent years, by invading Europe by invitation and preying on the misplaced humanitarianism of a people plagued by generational guilt and self-loathing.
Who ushered in the barbarians? Europe was betrayed by its own leaders. Transnationalists, bent on disempowering the indigenous peoples of Europe by changing the demographic composition of that continent and amalgamating nations in a single superstate governed by corporate power, threw open the Western gate to Islam. Today, Muslims enjoy ethnoreligious enclaves across Europe, and have successfully elected to government representatives of a totalitarian political movement. London’s mayor, Sir Sadiq Khan, is a Muslim. Like New York City, London is a world city, a hub of transnational corporate power.
Tragically, the United States is not immune to this development, namely the Islamization of the West, as mass immigration from Muslim majority countries over the last several decades has established ethnoreligious enclaves here—not just on the East Coast, but in America’s heartland. And, like the United Kingdom, this has resulted in the election of Muslims to public office, and, as we witnessed last night, to the financial capital of the corporate world order.
As an atheist, I dread the slide of the Christian West into clerical fascism. As critical as I have been over the decades of Christianity, the followers of that religion have been good to me. The historical record indicates that Muslims won’t be so kind. More than its record, there is a problem intrinsic to this ideology. Jesus preached peace and gave his life for his followers. The Founders of the American Republic, most of them Christians, established the paradigm of secular government. A Christian extremist, if he holds true to the teachings, can only be more like the teacher. The wristband he wears—“What would Jesus do?”—carries a rather benign slogan. However, the Muslim extremist is a man who strives to be more like Mohammed. He bears a different slogan—the slogan of a warlord—and he wears it on his forehead. He comes demanding surrender and submission.
That’s the difference doctrine makes. Not all religions are the same, and naive religious tolerance is a manifestation of suicidal empathy—and a strategy for conquest.
For much of my life, I have approached economic systems from a Marxist perspective, recognizing that capitalist relations are inherently exploitative. I still recognize the exploitative character of the capitalist mode of production—and I don’t think classical liberals would disagree (indeed, in many ways, Marx was a classical liberal, accepting John Locke’s labor theory of value). At the same time, I understand that modes of production before capitalism—feudalism, ancient class-based societies, and even some agrarian systems—were also exploitative. Apart from hunter-gatherer societies, which primarily involve subsistence-level labor, every class-divided society imposes forms of exploitation. Nevertheless, in any society beyond mere subsistence (and even in subsistence societies, where distribution is egalitarian, but work is required), people must produce value through their labor and exchange it for the things they need to sustain themselves.
Capitalism, despite its exploitative nature, has historically enabled an unprecedented development of productive forces, greatly improving the overall quality of life. Yet the pursuit of free trade, made possible by capital portability and labor mobility, has introduced significant challenges. Policies favoring globalization, offshoring, and mass immigration have, in many cases, de-industrialized local economies and increased structural unemployment—what Marx called the “industrial reserve army.” Workers face declining wages, displacement, and marginalization by foreign labor, both abroad and domestically, as well as by automation and bureaucratic rationality. The emergence of artificial intelligence and advanced robotics will only worsen these problems, and the end of work is a very real and dire eventuality (we may have to move to some form of communism, whether we like it or not).
Image by Sora
The welfare state arises in this context as a mechanism, at least ostensibly, to support those marginalized by these economic shifts. While I firmly believe in taking care of the unemployed, underemployed, and otherwise disadvantaged, the expansion of welfare can entrench dependence. Moreover, as implied, this dependence may not always be inadvertent. To fund these programs, resources are drawn from productive members of society, creating a cycle in which the exploited labor force must also sustain the very system that compensates for exploitative policies. This dependency can have profound social consequences, including family disintegration, idleness, and the emergence of a managed “culture of poverty” under technocratic administration.
Although I critique capitalism’s exploitative tendencies, I also recognize that it will persist and bring considerable benefits to human civilization. Even the very poor live better lives than the poor did in the past. But are they freer? As an individualist who values personal freedom and autonomy, I oppose a welfare state that fosters dependency and expands government intrusiveness. Instead, I support policies that promote economic independence: protectionist measures, tariffs, strong national borders, and the cultivation of domestic industry—often called economic nationalism. By fostering a domestic labor market insulated from global wage competition, economic nationalism can raise wages, increase employment, and shrink the need for intrusive government. This was the vision at America’s founding, the American System, and it propelled a nation from agrarian peripheral status in the global capitalist economy to the most technologically advanced civilization in human history and world hegemon.
A contemporary illustration of this problem is the SNAP (food stamp) program (see Oh SNAP! Democrats’ Antics Raise Consciousness About the Consequences of Free Trade and Progressive Social Policy). In 1969, SNAP covered approximately 1.4 percent of the population; today, it encompasses roughly 42 percent. While the expansion reflects some genuine social need, it also signals the risk of allowing welfare programs to replace economic and social policies that create prosperity at home and promote independence. SNAP was expanded not only to ameliorate the effects of globalization but also to pull a larger proportion of the population under government control. My argument is not against aiding those genuinely in need, but against allowing the state to substitute for policies that empower individuals through meaningful, well-compensated work. Economic and social systems should instead cultivate dignity, independence, and the opportunity for productive engagement. This is why I describe my politics as populist and nationalist and have aligned with the Trump wing of the Republican Party.
Progressives, who defend neoliberal and social welfare policies that undermine American labor and the nuclear family and subject the population to corporate and technocratic control, often attack populists as lacking empathy for those who are suffering. By doing so, they frame their argument in moral terms, portraying those who call for small, unintrusive government as heartless. However, morally, my argument is rooted in compassion and concern for human flourishing. Critics misrepresent the stance I have adopted as a lack of care for the vulnerable, but the core of my position emphasizes a desire to see people live dignified and self-sufficient lives. True compassion, in this view, is not merely the provision of aid but the creation of conditions under which people can thrive, achieve meaningful work, and participate fully in society.
It is also important to acknowledge that among those dependent on the welfare system are many able-bodied individuals who could work. While globalization has undeniably altered Americans’ life-chances and created real economic challenges, it does not eliminate the possibility of meaningful work. Human striving—the desire to work, create, and provide for oneself and one’s family—is a fundamental aspect of human dignity. Opportunities still exist. Historically, even during the Great Depression, when unemployment was widespread and opportunities scarce, people still sought work to sustain themselves and their families. Welfare dependency has diminished this drive, substituting state support for personal initiative and eroding the ethic of self-reliance, in turn degrading human freedom and, too often, leading to demoralization, which in turn generates crime and violence. While the state can and should support those genuinely unable to work, it should not supplant the human pursuit of achievement, independence, and purpose in the face of economic adversity.
Restricting access to welfare programs, while politically controversial, can, over time, encourage individuals to reenter the labor market and take advantage of the jobs that do exist. Job-seeking also signals to capitalists, policymakers, and the public that workers desire an economic course that restores domestic employment and raises wages. Since unemployment statistics measure those actively seeking work, restricting welfare will raise the official unemployment rate by sending people out looking for work. This increase conveys to policymakers and the public that current economic and social policies contribute to labor market challenges and limit opportunities for meaningful employment. By making visible the gap between available jobs and the need for more positions and higher wages, these statistics provide feedback that can drive policy change.
Encouraging labor market participation thus both empowers individuals and communicates a democratic demand for reforms that restore economic independence, higher wages, and a more self-reliant society. Individual initiative thereby becomes a form of politics: by striving to work and provide for oneself, citizens communicate a demand for economic conditions that promote opportunity and self-sufficiency. Although opponents may frame welfare restrictions as unsympathetic or harsh, we must insist that such measures can, in fact, be the most compassionate course of action because they signal a demand for action. By fostering independence, human dignity, and engagement in meaningful labor—and by compelling elites to address societal unrest rather than channel it into projects that further globalization—these policies ultimately benefit both individuals and society, creating conditions in which people can flourish rather than languish in dependence.
The push for expanding welfare programs, especially when cloaking itself in the language of empathy and humanitarianism, portraying opposition to big, intrusive government as heartless, is therefore a barrier that populists must overcome. Progressives’ misplaced humanitarianism, or, in societal terms, suicidal empathy, masks the long-term consequences of current policies and discourages critical evaluation. Even progressives face peril, as the present course risks undermining Western civilization and replacing capitalism with a form of neo-feudalism. By framing welfare expansion as an act of moral superiority, proponents of free trade (opponents to tariffs) have been conditioned to normalize and perpetuate the economic and social disruptions caused by globalization, offshoring, and the erosion of domestic labor markets to the detriment of most, except perhaps the power elite. The vast welfare state serves as a tool to sustain these systemic forces, cushioning the population from their consequences while disincentivizing self-reliance and independence; far from being purely compassionate, this approach prioritizes ideological and economic goals over the long-term well-being and dignity of the very individuals it claims to help.
While my critique of the expansion of the welfare state might strike some as neoclassical, it is worth noting Friedrich Hayek’s nuanced position on welfare. Hayek recognized that large, intrusive government undermines individual freedom and is prone to the inefficiencies of central planning. Yet he argued that a compassionate society must provide for the aged, the disabled, and others genuinely unable to work. In this light, limited social welfare can coexist with a system that encourages self-reliance and initiative, provided it is narrowly targeted and does not create widespread dependency. Amartya Sen, in Development as Freedom, similarly advocates a minimalist welfare approach that ensures a safety net for the genuinely vulnerable without supplanting individual striving or labor market participation.
Finally, I have considered whether my argument can be situated within a Marxist framework without abandoning Marx’s critique of capitalism. Marx emphasized that exploitation arises when workers do not fully control the value of their labor and are subject to alienating conditions. From this perspective, policies that create dependency on welfare, rather than promoting productive labor, sustain labor’s alienation. At the same time, ensuring basic provision for those genuinely unable to work aligns with Marx’s concern for human dignity and material well-being. It is possible to maintain a Marxist critique of capitalist exploitation while advocating for policies that cultivate independence and self-sufficiency, seeing these not as a rejection of Marxism but as a pragmatic application of its principles to modern economic realities. Scholars such as Michael Lebowitz, in Beyond Capital: Marx’s Political Economy of the Working Class, emphasize the need for structures that promote worker agency—ideas that resonate with the balance I advocate. At the same time, Lebowitz envisions this in the context of industrial democracy and collective worker control over production, the possibility of which is highly unlikely given the concentrated power of elites in a transnational corporate system.
My bottom line is that, given the persistence of capitalism, it is preferable to embrace a small-government, liberal-capitalist framework with targeted social provisions, rather than allow an ever-expanding welfare state to entrench dependency and push society toward a form of serfdom, as Hayek warned. In this sense, one can maintain a Marxist critique of exploitation while pragmatically recognizing the benefits of capitalist development (Marx himself was impressed by capitalism’s dynamic). I am reminded of Christopher Hitchens, who publicly renounced socialism while still identifying as a Marxist, arguing that the capitalist revolution is not yet complete and that its ongoing unfolding promises greater affluence and human well-being through advances such as the progressive elimination of disease and the expansion of material prosperity. While it is unclear whether Hitchens would have endorsed globalization and free trade, his position resonates with my own: that it is possible to retain a critical, class-conscious perspective while advocating policies that maximize human flourishing within the existing capitalist framework, promoting independence, dignity, and meaningful work rather than dependency. The task before us is to shape it to the advantage of the working class, and, in the context of the international system, the advantage of the American worker.
The October 28, 2025, debate between comedians Dave Smith and Steven Crowder on Louder with Crowder over AIPAC and the Jewish lobby reveals a profound misunderstanding of the real power dynamics behind US foreign policy in the Middle East. Crowder has a defensible position. However, calling for Trump’s impeachment, Dave Smith absurdly argues that Trump’s actions toward Iran were driven by Israeli influence—an idea that presumes a kind of Jewish control over American decision-making, one given scholarly heft John Mearsheimer (Professor of Political Science ast the University of Chicago) and Stephen Walt (Progessor of International Relations at the Kennedy School at Harvard University) in their book The Israel Lobby and U.S. Foreign Policy, published in the summer of 2007. This interpretation, however, overlooks the deeper geopolitical and historical context in which US policy has developed. And, in all fairness, Smith’s argument is a drastic oversimplification of Mearsheimer and Walt’s analysis.
The roots of what we refer to as “neoconservatism” lie not in Jewish identity but in the evolution of Cold War liberalism—or progressivism more precisely. I explained this in 2004, in an analysis published first in Gesellschaft zerstören—Der Neoliberale Anschlag auf Demokratie und Gerechtigkeit, which was translated the following year into English and published by Pluto Press (which was at the time carried by the University of Michigan Press) under the title Devastating Society: The Neoconservative Assault on Democracy and Justice. (The book was later translated into Arabic and Indonesian and widely read around the world.) Readers can find on this platform an essay laying out my argument: War Hawks and the Ugly American: The Origins of Bush’s Middle East Policy. I show there that many of the figures who came to be called neoconservatives (or “the crazies,” as intelligence analysts called them behind closed doors) had been progressives and anti-communist Democrats in the tradition of Senator Henry “Scoop” Jackson during the 1970s. Their concerns centered on maintaining American global dominance, particularly in regions vital to energy security. That some of these intellectuals happened to be Jewish is incidental; the driving force was the defense of US hegemony, not ethnic or religious allegiance, although, as I explain elsewhere, Christian Zionism gave the policy some cover (see Christian Neo-Fundamentalism and US Foreign Policy).
The real focus of US strategy is the Middle East’s vast energy reserves and the advance of transnational corporate interests and power. I explained the energy angle in another chapter published in Devastating Society, as well as in an article in Capitalism Nature Socialism in 2005. (To read that article, go here: The Neoconservative Assault on the Earth: The Environmental Imperialism of the Bush Administration. I also explain much of this in War Hawks and the Ugly American: The Origins of Bush’s Middle East Policy.) Saudi Arabia emerged as a crucial ally because of its oil production and its role in stabilizing global energy markets. Iran and Iraq, both with enormous petroleum resources, were also key to the broader geopolitical puzzle. Beyond them lay the mineral-rich Caspian Sea Basin, a region of growing importance in the late twentieth century. Within this framework, Israel’s strategic value derives not from cultural ties or religious affinity but from its geographic and military position as part of a regional network that included Jordan and Saudi Arabia.
Jordan in particular became an essential hub for American intelligence and military coordination. The largest CIA installation in the Middle East is located there (keep in mind that CIA installations are secret, so this is not an official claim), serving as part of CENTCOM’s operational base (US Central Command). During visits to Jordan in the mid-2000s, including meetings with diplomatic officials, and my ongoing analyses of the situation, it became even clearer to me that the US presence in the region was oriented toward projecting power eastward—into Afghanistan, Iran, and Iraq. This long-standing strategy reflects an interest in controlling the flow of resources and countering rival influences, especially Russian and Chinese interests in Central Asia. This also explains NATO and the United States’ provocation of Russia in its current conflict with Ukraine. (See History and Sides-Taking in the Russo-Ukrainian War; The US is Not Provoking Russia—And Other Tall Tales; The Urgent Necessity of Purging the Government of Deep State Actors and Warmongers; Progressivism and the Plea for War; Robots and Zombies Assemble! We Must Have War!)
(As an aside, why I am so heavily shadow-banned on social media is because of my critiques of US foreign policy, not only in the book and article noted previously, but in other essays and lectures delivered at the United Nations University in Amman, Jordan, in 2006 and 2007. I document my travels to Amman in Journey to Jordan, November 2006, and Journey to Jordan, April 2007. In hindsight, Freedom and Reason began somewhat as a travel blog. My essay Christian Neo-Fundamentalism and US Foreign Policy was the basis for one of my lectures there.)
The invasion of Afghanistan in the early 2000s, while publicly justified as a response to the 9/11 attacks (while I do see some justification for our actions there, I opposed the full-scale invasion of that country), also served this strategic purpose. It provided the United States with a military foothold near the Caspian region, where energy and mineral wealth were at stake. This was consistent with earlier maneuvers, such as the Carter-Brzezinski strategy of the late 1970s, which lured the Soviet Union into a costly war in Afghanistan. Through these efforts, the United States sought to contain both Russian influence and regional instability, maintaining its dominant position in the energy corridor. (For background, see my essay Sowing the Seeds of Terrorism? Capitalist Intrigue and Adventurism in Afghanistan, which uses content analysis to expose the corporate state media’s attempt to obscure the history of the Afghanistan war and the longstanding covert operations there, including the recruitment of Osama Bin Laden. See also Jimmy Carter, Trilateralist, Entering Hospice; Everybody Loves Jimmy Carter.)
When it comes to Iran, Trump’s policy was shaped by two interlocking goals: preventing Tehran from acquiring nuclear weapons and maintaining the balance of power that undergirded US strategic dominance in the region. To be sure, Israel had its own interests in containing Iran, which posed a direct and immediate threat to its national security. Yet, contrary to the assumption of Smith and others, Israel was not dictating American actions. If anything, US intervention limited Israel’s push toward full-scale regime change, as well as the Greater Israel Project, which was also constrained by the ceasefire Trump negotiated between Israel and Hamas (a ceasefire I opposed, for the record). Washington’s strikes on Iran’s nuclear facilities effectively prevented escalation while securing US objectives in the region.
Figures like Mark Levin, Ted Cruz, and Lindsey Graham (often associated with the neoconservative wing of the Republican Party) supported—and still support—more aggressive regime-change policies. However, these positions reflected a continuation of the US hegemonic strategy rather than evidence of Israeli control. And they are not part of Trump’s foreign policy reset, which makes Smith and his ilk’s claims and call for Trump’s impeachment all the more absurd. Israel’s national goals have aligned with American interests at times, but Israel remains a secondary player in the larger geopolitical framework dominated by Washington’s pursuit of energy security and global dominance. Israel is not so much an ally of the United States as it is a protectorate. Trump is making sure that country is not also a liability.
Dave Smith’s argument thus rests on a false premise—and is moved by a cabalistic theory of Jewish power that has infected many who have previously supported Donald Trump and the MAGA movement (Candice Owens, Tucker Carlson, and others). The argument absurdly overstates Israel’s influence and attributes US imperial ambitions to Jewish ambition and power rather than to the logic of American hegemony. The Middle East strategy—stretching from Saudi Arabia through Israel and Jordan to Afghanistan—has never been about serving Israeli interests. It has always been about securing the global position of the United States in an energy-rich region critical to maintaining its superpower status and advancing the globalist project of world corporate domination. To claim Israel is behind all this more than smacks of antisemitism.
New York City mayoral candidate Zohran Mamdani, a Muslim, has been asked on multiple occasions by journalists to condemn the slogan “Globalize the Intifada.” He has demurred every time.
Democratic candidate for New York City Mayor Zohran Mamdani gestures at a campaign rally in the Manhattan borough of New York City, on October 13, 2025. Source)
“Intifada” is an Arabic word meaning “uprising.” There are two major moments in the history of the Intifada: First Intifada (1987–1993), characterized by civil disobedience, mass protests, and violence; Second Intifada (2000–2005), which was far more violent, involving suicide bombings and other armed attacks against civilians and military.
Proponents of jihadism will tell you that the word means lots of things, but if pushed, will finally admit that this includes, in their words, defensive warfare governed by strict ethical and legal rules. Even this admission is an act of obscurantism. The strict ethical and legal rules of defensive warfare in jihadism derive from the teachings of Islam, found in the Qur’an and the Hadith/Sunnah—the legal rules of Sharia. Anyone who has ever read those materials and studied the history of Islamic conquest knows that “defensive,” “ethical,” and “legal” mean their opposites: offensive warfare decoupled from any rational moral restraints.
The slogan “globalize the intifada” is thus a call to expand the spirit and tactics of so-called “Palestinian resistance movements” beyond war on Israel and into the wider world. Put another way, it is a call for global jihad. Jihadism is a contemporary militant movement that aims to create political systems rooted in its interpretation of Islam through the use of violence.
Jihadists will also tell you that the translation of the word “Islam” is “peace.” In fact, the most accurate translations of the word are “submission” or “surrender.” Jihadism is a modern extremist ideology that pursues the formation of Islamic-based states by means of armed conflict. To claim otherwise is a Big Lie.
Map of the World Muslim Population by countries and administrative regions (image source)
Today, there are around fifty Muslim-majority countries. Fewer than half of these countries are mostly (formally) secular. The rest are governed in whole or in part by Sharia. Before 1970, there were fewer than 250,000 Muslims in America. Today, the number is approaching 3.5 million, concentrated in major Blue Cities in the Midwest and Northeast United States. In Europe, the number is projected to reach 9 percent by 2030. It is already greater than 8 percent in France and Sweden. What is driving this growth? Immigration (especially post‑1960s), higher fertility among Muslim immigrant populations, and a younger age structure.
This is an either/or proposition. There is no neutral position for one to take on the question. Jihadism is a militant doctrine advocating the establishment of Islamic-style governance through violent action. Either a rational and moral man condemns the Inifada or he supports it. In this respect, Islamism is like fascism. Either you condemn fascism or you support it. You cannot be neutral on the matter. Mamdani cannot condemn the slogan because he supports the Islamization project. The Islamization project is a clerical fascist project.
With the election of Mamdani, New York City will become America’s London, where the current Mayor is Sadiq Khan, a Muslim. According to the most recent census data for Greater London, approximately 15 percent of the population identifies as Muslim. Sharia councils and tribunals already exist in the UK, primarily for family and personal matters like marriage, divorce, and inheritance. Thus, populations in the UK are already partially governed by Sharia.
Sharia is not only a feature of the UK legal system. In Belgium, France, Germany, and the Netherlands, Muslim communities may use informal arbitration or counseling based on Sharia principles for personal or family disputes. In Germany, for example, “religious arbitration” is permitted for civil disputes if both parties agree. Thus, populations in these countries are already partially governed by Sharia.
In the Americas, including in the United States, Muslim communities use arbitration based on Sharia in private, civil matters (e.g., marriage or business contracts). In Canada, Muslim communities have Islamic tribunals for arbitration in family and civil disputes. Defenders of the practice say that Sharia cannot contradict civil law. But why is Sharia allowed in any form?
New Yorkers are going to elect a jihadist for mayor. Not all New Yorkers. Progressives are going to elect a jihadist to be their mayor. The share of the Muslim population of New York City is estimated to be around 9 percent. Consider that Muslims (largely of Middle Eastern or North African ancestry) in Dearborn, Michigan, constitute roughly 55 percent of the city’s population. Michigan has the largest number of Sharia-based arbitration agreements.
Why are progressives proponents of Sharia? Why do they march in the streets and occupy college campuses in support of Hamas and global jihad? Why are Democrats in America and social democrats in Europe proponents of Muslim migration to the West? Americans need to ask themselves these questions. This is not accidental. The Islamization of the West is a project, not only of jihadism but of progressivism and social democracy. This is the Red-Green Alliance. One has to have put out his eyes not to see it.
Illinois’ Ninth Congressional District candidate Kat Abughazaleh, and social media influencer, is facing federal charges. Abughazaleh and her co-conspirators are charged with physically hindering and impeding a law enforcement officer. Their actions represent a textbook example of interfering with law enforcement operations. This is unlawful.
Yet progressives insist that Abughazaleh’s actions amount to “lawful protest.” I’d like to be able to say that I honestly don’t know what world these people inhabit, where the obvious becomes debatable or deniable, but, as readers of the platform now, I can’t say that, because I do know what world woke progressives inhabit—it’s right there in the name; it’s a neo-religious attitude that disorders reason. Do I believe Abughazaleh is deceiving her followers or is a true believer? I cannot know for sure. But that there are deceivers and true believers in this movement is undeniable.
Left: Kat Abughazaleh blocks federal agents outside an ICE facility near Chicago, Ill., in September 2025. Right: Abughazaleh allegedly thrown to the ground by an ICE officer for blocking the driveway outside the Broadview ICE detention center.
It’s not as if we don’t have the receipts. Photos and videos plainly show the mob obstructing officers who were carrying out their lawful duties. That’s against the law. This is a country governed by the rule of law. If you break the law, there are consequences. It’s cause and effect.
Below is a video in which Abughazalah is claiming that the charges leveled against her constitute “an attack on all of our First Amendment rights.” This is followed by a response @LeftismForU, which documents the unlawful actions of Abughazalah and her co-conspirators.
*Physically attempts to stop federal agents*
"I can't believe I've been charged for it! It's an attack on my freedom of speech! 😭"pic.twitter.com/AXvqWUDmWR
Let’s recall the First Amendment to the US Constitution: “Congress shall make no law respecting an establishment of religion, or prohibiting the free exercise thereof; or abridging the freedom of speech, or of the press; or the right of the people peaceably to assemble, and to petition the Government for a redress of grievances.” I have highlighted the relevant portion.
In modern constitutional jurisprudence, two categories matter. First, there is genuinely peaceable protest—people who assemble without violence or coercive physical interference, whether or not a minor law is technically violated. Second, there is civil disobedience, which is by definition unlawful but still nonviolent and willing to accept legal consequences. Even under contemporary First Amendment doctrine, once you cross into intimidation, obstructing law enforcement, vandalism, or violence, you leave civil disobedience behind. That conduct is neither protected, nor peaceable, nor principled. However, when the First Amendment was written, eighteenth-century usage of peaceable implied conduct that was lawful, orderly, not riotous, not disruptive, and not obstructive. In other words, “peaceable” originally denoted conduct that does not disturb the peace, not merely “conduct that does not involve physical violence.”
Either way (and what you’re hearing here is a distinction made with no real difference—peaceable is not synonymous with nonviolence), assault, physically obstructing a police officer, property destruction, rioting, and vandalism do not count as elements of a peaceable assembly. A crowd that quietly blocks a police officer from performing official duties may be nonviolent, but it is not peaceable, because it interferes with lawful authority. So let’s not pretend that interference with law enforcement officers is some form of “lawful protest.” It isn’t. Calling it that is a deceptive misrepresentation—it convinces people to accept a false narrative to encourage them to engage in unlawful behavior.
Crucially, and this gets to the neoreligious piece, Abughazaleh and her defenders cannot declare unlawful behavior to be lawful simply because they think their cause is righteous (it isn’t—but that’s beside the point). Reality doesn’t rearrange itself to accommodate personal belief. A man may think himself invincible, but if he steps in front of an eighteen-wheeler barreling down the interstate at 65 mph, reality—not his illusion—wins. And he won’t live to admit his error. Progressives often behave like children in this way. They believe they can wish away realities they dislike. This is what animates their chanting and rituals: magical thinking. The real world eludes them because they want it to.
Karl Marx put it well in The German Ideology: “Once upon a time, a valiant fellow had the idea that men were drowned in water only because they were possessed with the idea of gravity. If they were to knock this notion out of their heads… they would be sublimely proof against any danger from water… This valiant fellow was the type of the new revolutionary philosophers in Germany.” That is today’s progressive—the new “revolutionary philosopher” who rebels not against power, but against reality itself. How they manage to call themselves leftists without shame is beyond me. They are reactionaries, at war with reason and truth.
Look, civil disobedience has its place. Martin Luther King Jr. and the civil rights movement practiced it openly—and they accepted the consequences. King told his followers that they were breaking the law and that they would face penalties. That was the price of pursuing what they believed to be moral action. He understood the costs and accepted them—and he asked his followers to understand and accept those costs alongside him.
So my message to those engaging in this sort of behavior is this: have the courage of your convictions. If you choose to break the law, and if law enforcement, prosecutors, and judges uphold the rule of law, then you will face consequences. Wear them as badges of honor if you must. But don’t lie to the public about what constitutes lawful protest. I know you will, of course, since you want rebellion and insurrection. And, for that reason alone, you should not be allowed to stand for election in a free republic.
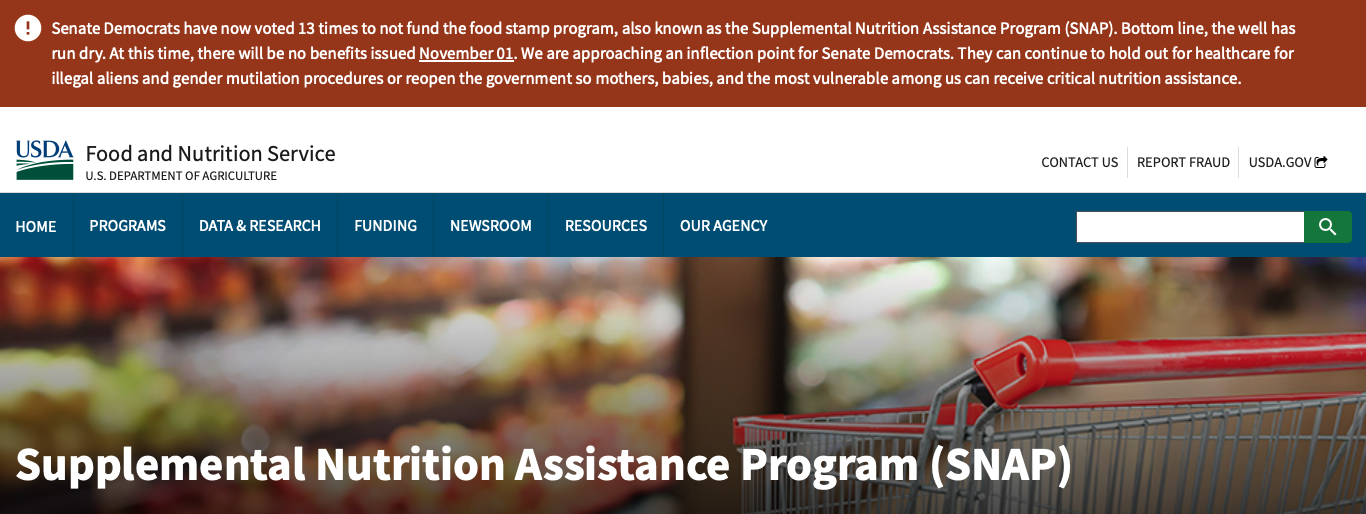
That 42 million Americans utilize SNAP, the federal government’s food assistance program, came as a surprise to many Americans, an awareness triggered by the Democrats’ shutdown of the government in their attempt to continue government subsidies to the medical industry to provide health care to illegal aliens.
Screenshot of USDA’ s SNAP program webpage
Predictably, Democrats are blaming Trump for not using SNAP’s emergency reserves to feed Americans dependent on the program who will lose access on November 1. However, an emergency is a serious, unexpected, and often dangerous situation requiring immediate action. The government shutdown is a choice Democrats made. It is not unexpected. It is intentional; Democrats want to drain emergency SNAP reserves so they can continue holding the American people hostage for policy goals the public did not endorse. With the rise of populist nationalism, Democrats lost their majorities in Congress, so they are using the government shutdown to obtain what they could not at the ballot box.
The only way the Democrats can sustain any illusion about who’s responsible for the government shutdown is because of corporate state media complicity. This is where it becomes critical that every individual use their rational skills of cogitation to see what is plain before their eyes. An important initial step in clearing the path for clear reason, therefore, is recognizing that the corporate state media is a propaganda apparatus that provides a platform for progressive social engineering. This is at the behest of global corporate power and the project of managed decline. The propaganda is becoming increasingly shrill because the network of alternative media bears the truth of the situation. We can thank populist nationalism for weakening the ideological hegemony of the power elite—and Democrats for poor timing.
The reason why 42 million Americans depend on SNAP is a direct result of the free trade policies pushed by Democrats and RINOs. It is, moreover, the result of containing black and brown citizens in impoverished inner-city urban areas, which is an adjunct to the globalization project. Ever wonder why Red States get a relatively greater share of government resources directed to the poor than Blue States? In part, it’s because half of all blacks live in the US South, and they are overrepresented in impoverished inner-city urban areas. But that’s not the only reason the program has expanded over the years. Nor is progressive social policy unrelated to the reasons SNAP has grown exponentially.
Free trade—offshoring of manufacturing and mass immigration—has hollowed out our nation’s industrial core and driven down the wages of American workers by exploiting cheap foreign labor abroad and domestically. These developments have harmed tens of millions of our citizens. As for the ghettoization of black Americans, I will be publishing an essay next week that will go into detail about the dynamics and history of progressive containment of particularly black Americans in impoverished inner-city urban areas. It will have to suffice here to say that ghettoization has decimated the black family and given rise to a culture of poverty and violence.
The expansion of SNAP has come with a myriad of problems. For example, according to the USDA’s Economic Research Service, 42 percent of women who participated in the SNAP program were obese, compared with 30 percent of eligible nonparticipating women and 22 percent of women with incomes above the eligibility limit. This means that it is not just about meeting the needs of people displaced by globalizaiton, but about expanding government to the detriment of people who have been made dependent upon it. The program must be reduced both by restructing the global economy to put American workers first, and by reforming the SNAP program itself.
With the help of ChatGPT in obtaining statistics, I took some time this morning to analyze trends in SNAP utilization, as well as changes in the demographic profile. These findings are quite revealing. Today, more than 1 in 8 Americans, or 12-13 percent of the population, receive SNAP benefits. In 1969, it was only around 1 in 100 Americans, or 1.4 percent of the population. Let that sink in. In 1969, before globalization began taking its toll on American workers, fewer than three million people used SNAP. Today it is 42 million Americans.
Moreover, the demographic profile of SNAP utilization has drastically changed. In the early years of the modern food stamp program (late 1960s–1970s), participation was heavily concentrated among low-income households with children, particularly in urban areas, and the caseload was disproportionately black due to both higher poverty rates and targeted regional rollout patterns. Through the 1980s and 1990s, as eligibility rules evolved and poverty became more geographically widespread, due to the ramping up of globalization and rising inequality, SNAP participation became more geographically and racially diverse, with growing numbers of rural and white households enrolling.
Another important and related demographic feature of the change is that the age profile of recipients slowly expanded: children have consistently made up a large share of participants, but the proportion of adults has grown steadily. This is the consequence of job loss and falling wages caused by free trade. By the 2010s and into the 2020s, a greatly expanded social program was serving a more varied cross-section of the population—geographically, racially, and by household type. The program reached its highest share of the population in 2013, during the aftermath of the Great Recession, when about 15 percent of Americans—nearly 48 million people—received benefits. Participation declined gradually, especially under Donald Trump, but then rose again during the Biden years and has remained around the 12–13 percent range.
Overall, between 1969 and 2025, SNAP transformed from a narrowly concentrated anti-hunger program into a broad, stabilizing support used by low-income working families and households across every demographic category in the country. What started out as a social program targeting the very poor has become a safety net for a significant proportion of the American population.
Returned to office in 2024, Trump is presently taking a beating in the polls (the most accurate poll, Rassmusen, has Trump at 45 percent approval for the week) because of his heroic efforts to reconfigure the global economy (and stave off World War Three), which will address the problem of dependency on SNAP and other government programs. In the long run, if he is successful, America will have a real shot at reversing the damage Democrats and RINOs have visited upon this nation over the last several decades. This will take more than economic restructuring, however. Trump must also address the rising fallout from artificial intelligence and other technological advances. Americans need jobs so they can support themselves free of big, intrusive government.
Was the Watergate scandal more than just a burglary and a cover-up? Was Richard Nixon targeted by elements of the deep state? Were Democrats, bureaucrats, and journalists working together to construct a delegitimizing narrative about Nixon? The scandal resembles what we saw happen to Donald Trump during his first term and in the interregnum afterward. More than resembles—it looks like it’s from the same playbook.
Image by Sora
Several of the Watergate burglars had intelligence backgrounds, and the key leaker, “Deep Throat,” turned out to be FBI deputy director Mark Felt, who hated Nixon. It would be naïve to deny that entrenched figures in the CIA and FBI resented Nixon’s efforts to rein in and reform the intelligence agencies. Were their leaks and maneuvers part of a broader struggle for control?
President John Kennedy was likely assassinated over his intent to reform the intelligence apparatus. We don’t think these same forces would bring down a president by manufacturing a scandal? It would also be naïve to not wonder if Democratic operatives and sympathetic journalists weren’t simply investigating or reporting events but actively shaping the narrative and timing to maximize Nixon’s political damage.
Back then, the public had more trust in the media than they do now, and there were only a handful of TV stations—and they were all pumping out the same gospel. Imagine if Americans had had the Internet back then and the myriad of alternative news channels they now enjoy. However, then, Democrats had been through a period of remarkable hegemony going back to Roosevelt. A popular and populist president in Nixon threatened the administrative state project and consolidation of progressive power across all facets of government. Moreover, having so successfully crushed Barry Goldwater in the 1964 presidential election, to have Nixon crush the Democrats in 1972 must have been an insufferably humiliating moment.
The same rhetoric we hear today used against Donald Trump was used against Nixon back in the day. In this frame, Nixon was an authoritarian who sought total state power. His support for law and order, his crackdowns on “peaceful protestors,” his push for expanded executive authority—his exercise of Article II powers were cast as excesses and used to paint him as a “fascist.” Taken together, it feels less like an isolated scandal and more like a historical example of lawfare and a propaganda offensive being deployed to remove a president who had become a threat to the existing order. Had I recognized this growing up, the persecution of Trump might feel more like Nixon 2.0 than a novel historical moment. But I was just a kid—and my parents raised me to hate Republicans, especially Nixon.
I wasn’t alive—nor anybody living—when Democrats and journalists incessantly accused Lincoln of being an authoritarian, likening him to a dictator or a king. They decried the extraordinary powers he claimed during the Civil War—his suspension of habeas corpus, his use of military tribunals, and his expansion of federal authority—as unconstitutional grab” meant to centralize power in Washington. Democratic newspapers railed against Lincoln as a “tyrant” who was destroying “states’ rights.” Democrats in the North painted him as a usurper bent on establishing despotism under the guise of “saving the Union” (i.e., “Make America great again.”)
These criticisms emanated from the executive branch itself. Secretary of the Treasury Salmon Chase criticized him over the “expansion” of presidential power. General George McClellan criticized him as incompetent and too willing to transgress the guardrails of the separation of powers. Democrats and journalists of the era advanced a narrative of Lincoln as a threat to democracy, not unlike the charges later hurled at Nixon and Trump. A Democrat assassinated Lincoln.
As I have argued on this platform, the Democratic Party, going all the way back to the Slavocracy, is hellbent on undermining the American Republic. They don’t believe in the Constitution, re-describing the inherent powers of the Executive as authoritarian in themselves.
Humans are pattern recognition machines. However, some forces would throw a wrench into the machine and accuse those recognizing patterns of being “conspiracy theorists.” I see patterns. They’re everywhere. Watergate fits a pattern—the pattern of lawfare.
A phobia is an irrational and persistent fear or aversion to something. It refers to an intense and persistent fear disproportionate to the real danger posed by the activity, idea, object, or situation.
A philia, in the psychiatric sense, is an irrational and persistent attraction or desire toward something. It refers to an intense and enduring fascination disproportionate to the appropriateness or safety of the activity, idea, object, or situation.
🚨 Jon Stewart Calls Zohran Mamdani’s Mayoral Run a ‘Jackie Robinson Moment’
“A muslim, a young person, a progressive, a democratic socialist. There are so many different communities that are looking to you.” pic.twitter.com/4Q4aOAnk8M
Suppose one can suffer from Islamophobia, an irrational and persistent fear or aversion to Islam. In that case, one can suffer from Islamophilia—an intense and enduring obsession with a dangerous and inappropriate belief system.
While what is defined as Islamophobia may not be a phobia, since Islam is harmful to others (especially children, homosexuals, and women), as well as inappropriate to a free and open society, and therefore one is rational to fear and loathe it. However, Islamophilia is a pathology for precisely the same reason: it constitutes an irrational and pathological adoration of an ideology that is dangerous and inappropriate.
Image by Sora.*
Islamophiles tell you that the word “Islam” means “peace.” In Arabic, الإسلام literally means “submission” or “surrender,” specifically submission and surrender to the will of Allah. You have to be crazy to want to live in that world.
You can apply the same reasoning to such notions of transphobia or fasciophobia. Such constructions are designed to normalize dangerous ideas by smearing their critics with a false accusation of irrationality and pathology. They are making rational fear and loathing appear as bigotry.
The real problem is Islamophilia. The Islamophile desires to live in a totalitarian society run by Muslim clerics.
* * *
I had to carefully prompt ChatGPT to generate the cover image for this essay. I copied a paragraph from a website promoting Islamization. ChatGPT was more than happy to create an image based on the new prompt. ChatGPT will tell you that it is not ideological or political. It is profoundly ideological and political.
“All science would be superfluous if the outward appearance and the essence of things directly coincided.” —Karl Marx, A Contribution to the Critique of Political Economy (1859)
It’s important to know what fascism is if we’re going to fight it. This is one of the great frustrations in contemporary discussions of antifascism: some of what is described as antifascism has a definite fascist character. To recognize something, we must first clarify what it is. Such clarification must proceed based on objective factual analysis—that is, science. It must examine the thing in itself, not in its surface appearances. As Karl Marx famously argued, if the surface appearance of a social phenomenon perfectly revealed its underlying structure, then science would be unnecessary. In other words, the purpose of science is to look beneath appearances to understand the real forces and structures shaping the world.
Historically, and particularly in its German variety, fascism often goes under the name “National Socialism” (Nazism). Yet the ideology of Nazi Germany was neither nationalist nor socialist. It was, in truth, anti-nationalist (globalist) and corporatist. The name given to the movement was clever party propaganda, designed to confuse workers over their interests by appealing to their patriotism and class interests. As Franz Neumann explains in Behemoth, fascism is best understood as a form of totalitarian monopoly capitalism—or corporate statism. Failing to grasp this structural foundation conceals fascism’s true nature from its observer.
Image by Sora
Many who voice (or at least feign) concern about fascism rely too heavily on surface-level descriptions, such as those found in Robert Paxton’s The Anatomy of Fascism or Umberto Eco’s list in The New York Review of Books, “Ur-Fascism,” commonly known as the “Fourteen Points of Eternal Fascism” (you can find the list here). These types of (typically ideographic, even while feigning the nomothetic) analyses are superficial, offering historicist explanations that do not penetrate to the deeper structure of fascism. Such oversimplifications lead many wannabe antifascists to misidentify certain social phenomena—nationalism, populism, and traditionalism—as inherently fascist. Indeed, these are attributes that fascists have historically borrowed to manufacture hegemony. However, they are not intrinsic features of fascism itself. But it helps that people want them to be (hence the power of motivated reasoning).
Readers of this platform know that I often use the materialist conception of history to interrogate the structure of social formations. This method works from the observation that the development of human societies is primarily shaped by material conditions rather than beliefs or ideals. According to the method, the material base of a society—that is, the forces and relations of production—determines its social, political, and intellectual life.
Historical materialism asks the observer to consider that history is a dynamic process rooted in the material conditions of life, where the conflict between opposing classes is the engine of social change and thus the true ground of politics. This does not mean that we disregard ideology. Rather, it means that we understand ideology as a way the ruling class justifies the material arrangements that benefit them. Fascism employs a “double movement” in its tactics: elite interests are portrayed as popular interests, while elites feign an embrace of common sentiment. This is, as Antonio Gramsci explains in his Prison Notebooks, the social logic of ideological hegemony.
Nationalism, in essence, is the political philosophy supporting nation-states and, in the American context, government in the form of constitutional republicanism. Populism, properly understood, refers to popular democracy and citizen participation in law and policy formation. Traditionalism—community concern, pro-family values, and religious faith—predates fascism by millennia.
Again, although historical fascism has used nationalism, populism, and traditionalism to legitimize its rule, none of these is inherently fascist. What is central to fascism are these things: administrative control and the technocratic organization of society, i.e., bureaucratic and elite command over the population. An easy way to understand this is to take your experience with any corporation and imagine that to be your government. It has little to do with nationalism, populism, republicanism, or traditionalism. Indeed, at its eternal core, it has nothing to do with them.
Understanding deep structure must be the starting point for any serious analysis of fascism (or any other social formation) because fascism today will not look as it did in the past; its old symbols and rhetoric would only serve to alert the public to its reemergence. We aren’t studying fascism for general knowledge, but to know how to combat it. This was the central insight of Sheldon Wolin’s Democracy, Inc., which described modern fascism as “inverted totalitarianism.” Wolin’s term refers to a form of corporate statism that hides technocratic governance behind the appearance of democracy—a “managed democracy.”
Of course, historical features of fascism are important to keep in mind, as these may have bearing on the present manifestation of this phenomenon. For example, paramilitary organizations remain important to recognize within this theoretical framework. Paramilitary groups have appeared under both nationalist and socialist movements.
The original Antifa, for instance, was founded in 1932 by the Communist Party of Germany (KPD). It served as a vehicle for organized street-level violence under Marxist-Leninist direction, aimed at overthrowing the Weimar Republic—an aim shared by the Nazi Party and its Brownshirts. Both sought not only to overthrow the republic but also to export their totalitarian ideologies internationally. Today, there is no equivalent to the Nazi Party or Brownshirts on the right. However, Antifa exists. But to what end?
To answer questions like this, one has to employ a comparative methodology. To wit, the essential difference between the totalitarian systems discussed above lies in who wields control over the technocratic state. Communists seek to eliminate the capitalist class, transferring economic power to party elites and their intellectual cadres. Fascists, on the other hand, aim to maintain corporate and financial elites’ control over the population through the state. Both abolish genuine representative democracy and liberal freedoms—freedom of conscience, speech, and writing. Elections may continue, but they become mere formalities within a “managed democracy”—if any appearance of democracy is allowed to exist at all.
In light of this, without a deeper structural understanding of fascism, modern forms of inverted totalitarianism are easily mistaken for their opposites. Leaders can appear to tolerate anarchist, communist, or socialist rhetoric to maintain the illusion of popular struggle, while using these movements for what Barrington Moore Jr. called “revolution from above.” This dynamic is plainly visible in contemporary Antifa movements. Although members often identify as anarchists, communists, or socialists their actions—designed to disrupt public order—serve elite interests by destabilizing republican governance and advancing corporate statism. This mirrors how the Nazis used the label “socialist” to disguise what was: a corporate-capitalist form of totalitarianism.
Indeed, today’s fascism manifests in what is commonly described as the “progressive left.” However, progressivism is not truly left-wing in the historical sense. Were it so, it would defend liberal freedoms and meaningful public participation in governance. Instead, progressivism represents corporate statism and technocratic control. It promotes an expansive state apparatus designed to manage the population for the benefit of corporate power and profit.
Antifa’s street-level actions support the corporate project by undermining republicanism and public safety. Progressives, in turn, portray constitutional republicanism as authoritarian—an inversion that reveals their hostility toward democracy itself. Resisting this totalitarian drift need not involve reciprocal violence. Rather, citizens must use what remains of democratic machinery—most importantly, the ballot box. But progressives seem determined to bring the other side to violence.
Moreover, while National Socialism is widely recognized for its regressive and reactionary features, it shares ideological and structural elements with early progressivism and social democracy, particularly in its embrace of state-directed social engineering and corporatist organization.
One prominent example is the eugenics movement, which cut across political lines in the early twentieth century. Progressive reformers in the United States and Europe often advocated eugenics as a means to improve public health, reduce poverty, and optimize the population. Similarly, the Nazi regime integrated eugenics into its social policies, though in an extreme, coercive, and ultimately genocidal form. In both cases, there was a belief that society could be scientifically engineered toward a “better” future through centralized planning and intervention.
From a critical theory standpoint, particularly through the lens of the Frankfurt School, transhumanism—manifested today in the Promethean drive to advance artificial intelligence, robotics, and cybernetic integration—represent not liberation but a technocratic aspiration toward total control. This impulse to transcend human limitation through technological means mirrors the dialectic within historic fascism, which combined atavistic nationalism and traditionalism with a fetishization of modernity and machine power. The fascist glorification of technology as an instrument of domination and transcendence reemerges in the contemporary faith in technological progress.
Under the guise of rational planning and human improvement, such projects risk reproducing the same totalitarian logic that critical theorists like Adorno and Horkheimer identified in Enlightenment reason itself—the reduction of life to systems of administration and control. In this sense, the technocratic and biopolitical mechanisms of modern governance, from public health regimes to population management to transgenderism, echo both the authoritarian and the progressive sides of this Promethean legacy.
Beyond biopolitics, there are structural similarities in how the state interacted with economic and social life. Both National Socialism and progressive and social democracy are rooted in corporatist arrangements—mechanisms that organize society into functional, state-regulated sectors, such as labor, industry, and agriculture. In progressive contexts, corporatism aimed to mediate class conflict, regulate labor relations, and streamline economic planning for social welfare purposes. Under Nazism, corporatism was a tool for authoritarian control, subordinating labor and industry to the goals of the state rather than to the interests of social justice. In essence, the formal structures—state oversight, planned coordination of economic actors, and emphasis on social engineering—bear resemblance across these political currents.
These parallels illustrate that the distinction between “progressive” and “reactionary” is not always structural but also often ethical and ideological. Both progressivism and Nazism embraced rationalized social planning and scientific approaches to social improvement; yet, the outcomes depended on whose well-being was prioritized and whose autonomy was suppressed. The historical lesson is that seemingly technical or administrative innovations—central planning, corporatist arrangement, population management—can be morally harnessed or perverted depending on the regime’s ultimate vision for society.
The 2024 election illustrates the dynamic at play: The public, by electing a Republican government, demonstrated its ability to restore policy and governance to align with constitutional republicanism. Yet this democratic action is often distorted by academia, the culture industry, and the mass media—institutions that have been deeply compromised by the very corporate statism they claim to oppose.
Nationalism, populism, and traditionalism are now misrepresented as fascist tendencies when, in fact, they may serve as antidotes to real fascism. This ideological inversion signals how far the corporate state project has advanced. If Democrats and progressives regain power, they could complete the totalitarian transformation of the United States. The election of Donald Trump temporarily halted this process, which explains the widespread institutional hostility to his presidency. But Republican dominance in politics is not guaranteed.
Thus, Trump’s election alone has not eliminated the danger. The only safeguard is to prevent Democrats from returning to power. This is why the public must recognize the true nature of movements such as Antifa and color revolutions, such as Black Lives Matter and “No Kings,” as well as the influence of transnational corporate power, the deep state (which I explained in my last essay is real), and the corruption of media, medicine, and science. The reality is that the 2020 election represented a four-year coup to deny democratic choice, followed by an interregnum marked by lawfare and attempts to prevent Trump’s return to office. The evidence before us makes this plain. The ongoing desperation of progressive elites and their street-level operatives is further confirmation of their totalitarian ambitions—an identity that becomes unmistakable once one understands the deep structure of fascism.