
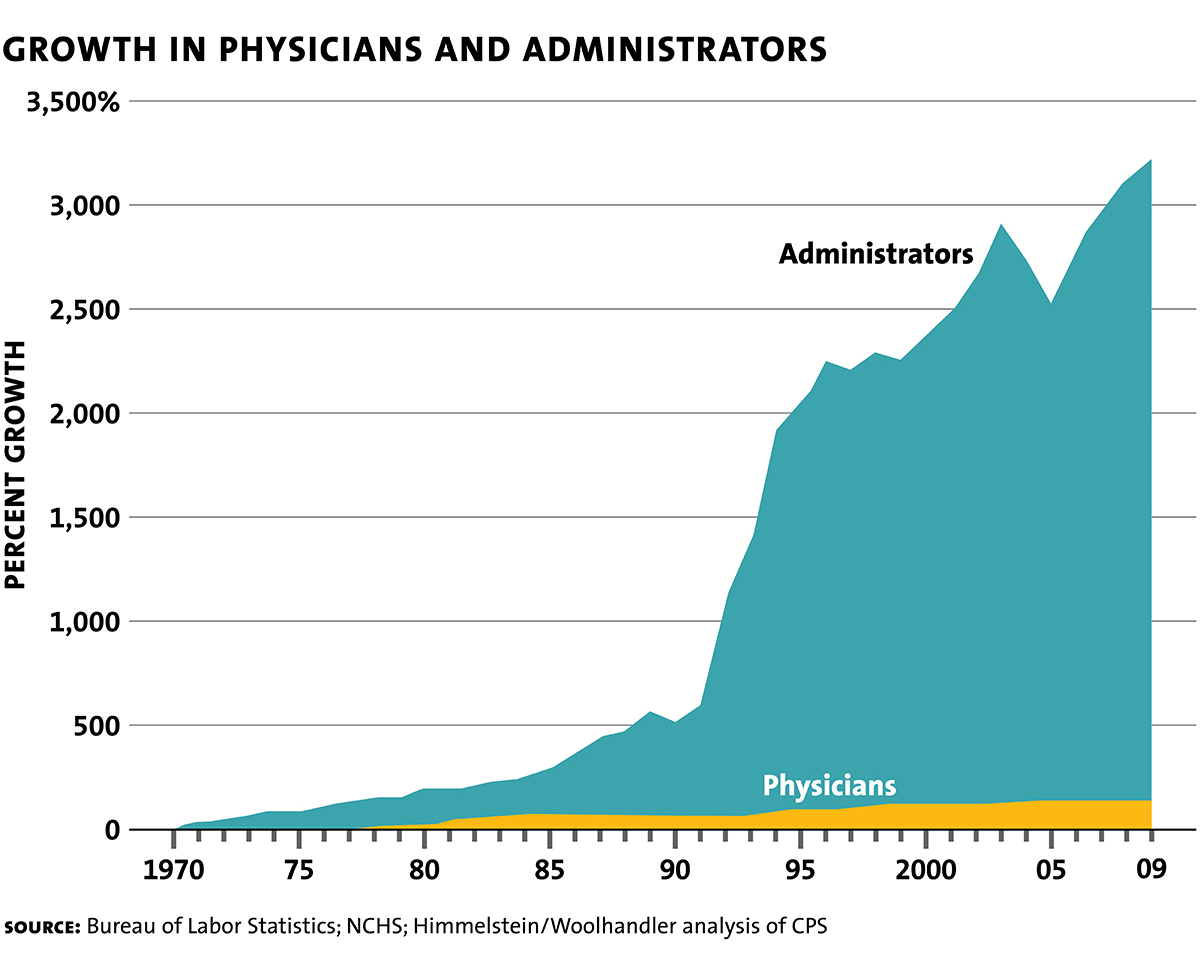
There are charts one can find on the Internet with later endpoints, but the chart I share below is clean and high quality. All the charts show the same pattern, anyway. Would it surprise readers to know that the ratio between doctors and administrators is even greater now? I am sharing this to encourage you to think about a few questions: What is the relationship of doctors to the medical-industrial complex? What is the role of administrators? What is the medical-industrial complex?
What I putting down here this evening is something of a follow up to my blog from a few months ago Making Patients for the Medical-Industrial Complex (see also my Disordering Bodies for Disordered Minds). This is also preview from an upcoming blog I’ve been working on concerning the intersection of queer theory and sexology, an ideology that is used to justify what the complex called “gender affirming care.” That blog is a lengthy one and what you will read here is some of a section that pulls things together towards the end. However, it stands alone as an analysis of that premise is known.
I ask in that forthcoming piece how one might consider the power dynamics embedded in social institutions and norms, and how these impact the lived experiences of individuals with non-normative sexualities and genders, by considering the following questions from above, repeated here for your convenience: What is the relationship of doctors to the medical-industrial complex? What is the medical-industrial complex? What is the role of administrators in this complex? In contrast to the postmodernists, who eschew objective analysis, I will answer the question from the scientific standpoint of historical materialism or critical political economy.
The medical-industrial complex is made up of a network of corporations that ultimately determines what counts as disease or medical conditions, what causes disease or medical conditions, what counts as treatments, and so forth. These are determined according to the imperative to accumulate capital, to generate income for investors and stockholders. The network of health care companies are intertwined with the network of health insurance companies, medical supply and technology firms, pharmaceutical companies, and the corporate-captured regulatory bodies that legitimize the system by appearing to monitor the behavior of the system for its benefits, efficacy, and safety. The health care industry generates somewhere in the range a trillion dollar annually. Two-thirds of the industry’s revenue comes from patient care. This makes generating more patients a lucrative business.
Administrators are bureaucrats of various rankings who run the hospitals and clinics for the network of corporations. Doctors are highly paid employees of the complex who, while appearing to have a significant degree of autonomy, are governed by the bureaucrats, their work rationalized by their schemes. Along with the engineers and scientists who work across the complex, doctors represent expert labor, with some in an expert management position. As employees and managers, doctors do the bidding of their corporate masters, a bidding many are eager to do because of the compensation—at least the amount of money they’re paid assuages the guilt those with a working conscience might otherwise feel exploiting the masses. The training they receive in accredited universities that dispense medical degrees is shaped by an ideology (“medical science”) determined by the apparatus of the complex—all this for profit generation. The more doctors push (unnecessary and dangerous) drugs, (unnecessary and dangerous) surgeries, and so forth, the more income is generated for the investors and stockholders. And so administrators push doctors to push these things.
As noted, because of the profit motive, health care companies are always on the prowl for more customers, and that means not only medicalizing more domains of human life, i.e., creating more diseases and conditions, but also aggressively diagnosing and treating the diseases and conditions they manufacture (the subject of the previous blog I reference above). For example, introduced in 1980 in the third edition, “gender identity disorder” (GID) was included as a diagnostic category in the Diagnostic and Statistical Manual of Mental Disorders (DSM-3), which legitimized a new frontier for the complex. The DSM-5, published in 2013, introduced significant changes to the diagnostic criteria and terminology related to gender identity. In fact, the diagnosis of GID was replaced with “gender dysphoria,” or GD. The change from GID to GD depathologized gender identity and the focus was shifted to the distress or discomfort individuals claimed to experience due to a mismatch between their gender identity and their birth sex.
But what explains the introduction of gender identity disorder in the first place? According to the progressive narrative, during the 1970s, there was a growing recognition among mental health professionals that individuals who experienced distress or dissatisfaction with their assigned sex at birth and identified strongly with the opposite gender may benefit from specialized clinical attention—and the mental health industry could benefit financially from finding more patients with this condition. This recognition was influenced by the field of sexology, which advanced John Money’s invention of “gender identity” (this is the subject of the upcoming blog). Trans activists agitated for the inclusion of gender identity in the DSM: if they could get their desire to transition recognized as a psychiatric disorder, then doctors could prescribe hormones and conduct surgeries and insurance companies could pay for some or all of it. The inclusion of GID in the DSM-III was pitched as a progressive step toward acknowledging and providing a framework for addressing gender-related concerns within the mental health field. In reality, it opened a new area of profit generation for the complex. Once the transgender care pipeline had been established and normalized, GID was depathologized and gender dysphoria introduced, which came with more benefits for the complex. (Again, all this is dealt with in much greater detail in the upcoming blog.)
The point is that more patients are made this way and in many other ways and, in many cases, made patients for life because disease or conditions are caused by the treatment, and the treatment regime is a terminal one. This is especially true of so-called gender affirming care. More generally, the complex is vast and injures and kills millions of people annually (estimates indicate that, depending on how you define medical error, 250 to 500 thousand people are killed every year from medical error alone, and many times that are injured). Both sexology and queer theory rationalize as a progressive project to promote inclusivity and acceptance of diverse sexualities and genders the generation of corporate profits, and they do this by dissimulating the reality of pain and suffering in the practice of carving fetishes into flesh with quasi-religious rhetoric of “authentic selves.” Psychiatry have created many more paths to profit than this, as readers probably already know. Tranquilizers minor and major, anti-depressants, anti-psychotics, etc. I have only scratched the surface. The revenue generated by the greater system is much greater that the trillion dollars hauled in by the health care industry.
